I’m going to reference Scapular winging: anatomical review, diagnosis, and treatments often.
–
Anatomy of scapular winging (muscular)
Serratus anterior
Of course, we have to start with this muscle.

The serratus anterior protracts and upwardly rotates the scapula.

Let’s use a nice quote from the paper to get more specific. Pictures and bolding from me:
“The serratus anterior is a broad flattened sheet of muscle originating from the first nine ribs and passes posteriorly around the thoracic wall before inserting into the costal surface of the medial border of the scapula.
(Fancy talk for it goes from the ribs to the scapula.)
The serratus anterior has three functional components. The superior component originates from the first and second ribs and inserts into the superior medial angle of the scapula. This component serves as the anchor that allows the scapula to rotate when the arm is lifted overhead.
The middle component of the serratus anterior originates from the third, fourth, and fifth ribs and inserts on the vertebral border of the scapula, serving to protract the scapula.
The inferior component originates from the sixth to ninth ribs and inserts on the inferior angle of the scapula. This third portion serves to protract the scapula and rotate the inferior angle upward and laterally.
As a whole, the main function of the serratus anterior is to protract and rotate the scapula, keeping it closely opposed to the thoracic wall and optimizing the position of the glenoid for maximum efficiency for upper extremity motion.”


It’s not just about the serratus anterior
The serratus anterior is not the only muscle impacting a winging scapula. When a scapula wings it’s because it isn’t held close to the rib cage. The serratus anterior gets a lot of attention because it’s anterior to the scapula, and attaches to the scapula. When a scapula wings it often displaces posteriorly. Naturally, the thinking goes the serratus anterior is “long and weak” because the scapula isn’ t being held close to the ribcage.
However, other muscles connect anterior to the scapula, and connect to the scapula.
Trapezius

Because the spine is ventral to (in front of) the scapula the trapezius can pull the scapula a bit anteriorly. That is, closer to the ribcage.
Parts of the trapezius also fall on top of the shoulder blade.

If the trapezius is on slack, or not firing properly, the compression on the scapula lessens. Making it more likely the shoulder blade won’t be as tight to the ribcage, aka wing.
Rhomboids
For many of the same reasons above, the rhomboids can play a role in the shoulder blade winging too. Because this is so rare (the authors go over this too), I’m not going to cover it.
Position of the scapula
Due to the attachment sites of the above muscles, we can get a good feel for which muscles need work by the position of the scapula. A nice chart from the paper:


Right scapula front view.

Right scapula back view.
Right shoulder winging due to issues with the serratus anterior (it gets progressively worse):
–
See how the scapula is traveling excessively medially and superiorly?


Winging due to issues with the trapezius:

From the paper: “Notice the lateral displacement of the scapula with the superior angle more lateral to the midline than the inferior angle.”
An important note here: I don’t think it’s feasible to fully separate these two impairments. When a serratus anterior issue is present it’s pretty much guaranteed there’s an issues with something like the trapezius. For instance, while this has serratus issues:
You can see issues with the trapezius as well. The superior angle (where the trapezius attaches) is lateral to the inferior angle. A sign the trapezius is also not firing like it should be.

–
Anatomy of scapular winging (nerve)
Long thoracic nerve
Much like the serratus anterior, of course we have to go over this nerve. The long thoracic nerve is part of the brachial plexus.

The brachial plexus is a group of nerves which run down from the neck, under the clavicle, connecting to various points around the shoulder. 
-Image credit and copyright to Kenhub (great anatomy site!)
The long thoracic nerve connects into the serratus anterior:


Because this nerve is what gets the serratus anterior to fire, and people with scapular winging often have so much trouble getting their serratus to work, the long thoracic nerve gets a lot of attention. However, attacking the nerve doesn’t get us anywhere. We need to go after why the nerve has a problem. Why is it having trouble firing, thus the serratus anterior is having trouble firing. The nerve doesn’t just sporadically stop working one day.
–
Figuring out the cause of scapular winging
“The serratus anterior is weak” is not a cause. “The long thoracic nerve isn’t working” is not a cause. Why are there issues with the serratus anterior? Why did it become weak? Why is it not firing properly? Why is the long thoracic nerve not helping?
Muscular
As I went over above, we’re primarily interested in getting the trapezius and or serratus anterior to work better. Muscles which help hold the scapula to the rib cage and lift (rotate) it upwards. With that, it’s logical to assume muscles which perform the opposite functions -pull the scapula away from the rib cage and or rotate it downwards- are likely working too much. Muscles such as, but not limited to, the rhomboids or pec minor. We want to calm them down. If they’re too active they can limit the ability of the trapezius and serratus anterior to do their jobs.
Nervous
We’re interested in anything which could limit the ability of the long thoracic nerve to fire. We’re primarily concerned with compression of the nerve. From the paper (when discussing the long thoracic nerve):
“Proposed vulnerable sites for injury include compression of the nerve between the clavicle and first rib and traction within the nerve’s fascial sheath.”
The clavicle and first rib may come closer together pinching the long thoracic nerve between them.

In my experience, this most often manifests with the clavicle / shoulder drooping.

Which goes hand in hand with our discussion of muscles pulling the shoulder down. The overactive muscles which may cause a shoulder to droop, are the same muscles which oppose the serratus anterior and trapezius.
This is the long way of saying you can’t really separate nerve issues from muscular issues. They work together. Granted, I once saw a woman who had her long thoracic nerve severed because of a mastectomy. Her winging was truly a nerve problem. But that’s the rare case. We’re more concerned with our average person.
So, how do these certain muscles become dominant? How does this nerve get compressed?
–
Daily activities causing issues with scapular winging
I’m going rattle off a bunch of scenarios where the shoulders are being depressed / downwardly rotated.
Bra Straps
The downward pull of bra straps can cause the shoulders to become depressed over time.

This is especially poignant for those who carry a considerable amount of weight in their bra.
Carrying heavy objects

Much like the bra strap comments.
Computer Posture
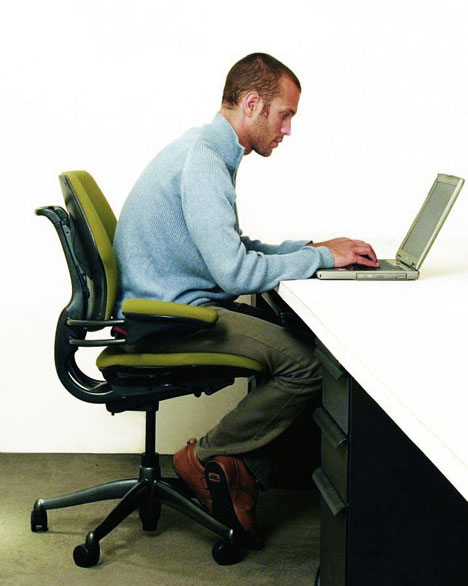
The forward head posture causes the levator scapulae (downward rotator) to pull on the scapula
The internal rotation (hands / arms turned down and in) can cause stiffness in the pecs and lats. Both of which can limit our ability to get our arms up.
Leaning on elbows

Notice the right shoulder protruding
This can push the shoulder into retraction, stiffening the rhomboids.

Next, this can indirectly cause winging. When leaning on the elbows the humerus can become displaced anteriorly (forward) and or superiorly (upward), lengthening the subscapularis.

A muscle which depressed the humeral head, pulling it posteriorly (backward) and inferiorly (downward).
When the subscapularis is lengthened it may shut down causing other humeral head depressors, such as teres minor and infraspinatus, to work more than they should.

These muscles can then stiffen up. This stiffness may appear when someone internally rotates their arm. Notice the winging during internal rotation here:

Credit to Diagnosis and Treatment of Movement Impairment Syndromes (Great book!)
I didn’t go over this in the initial anatomy section, but stiff external rotators of the humerus can cause winging as well. Because these external rotators connect 1) anterior to the scapula and 2) to the scapula, similar to the muscles I went over earlier. The difference being these muscles internally rotate the scapula (away from the ribs), while the others externally rotate it (close to the ribs).

–
Standing with hands on hips

This goes hand in hand with the above. The internal rotation causes issues with the lats and pecs, and the elbows behind the humerus promote anterior translation of the humeral head (stretching the subscapularis). All these muscles pull the arm downwards as well. Something we want to avoid in exercise too.

–
Exercise routines causing issues with scapular winging
Too much pulling
Exercises such as DB rowing, chin ups, lat pulldowns, chest supported row, all work on muscles which downwardly rotate and retract the scapula, as well as extend the humerus. Muscles like the rhomboids, lats, teres minor and infraspinatus. As we’ve seen, if anything, in someone with scapular winging we want to atrophy these muscles.
Too much work in horizontal plane
Horizontal meaning the arms move forward (in front of body) and back (behind body), rather than up (overhead) and down (below head).
Going with that, horizontal pushing exercises, such as push-ups, bench pressing, DB bench pressing, all work the pecs to a great degree. Muscles we again want to calm down.
Yes, it’s true some scapular protraction is present. But this is where we go back to the function of the serratus anterior.
“the main function of the serratus anterior is to protract and rotate the scapula”
And there’s minimal, if any, upward rotation in any exercise only taking place in the horizontal plane. Now we can see why something like the push-up plus exercise is pretty much futile.


Some people will lift the arms up a bit higher to place the shoulders in more of an upwardly rotated position. If you want to really upwardly rotate the scapula you know what you could do even more of? Lift the arms higher. Like, all the way up. Isn’t this the goal anyways? To be able to lift the arms all the way up?
Furthermore, exercises like the push-up plus and others may promote scapular protraction while simultaneously promoting scapular retraction.


–
Whatever you may be promoting in scapular abduction (protraction) you’re offsetting with adduction (retraction). Something you rarely want in a scapular winging issue, or most shoulder issues for that matter.
Note the similarities:
Pain during arm elevation due to excessive scapular retraction:
Looks pretty similar to the position of a push up plus:


Sure, you could cue around this (I rarely ever see someone do so), but you still have to account for the fact upward rotation is not being sufficiently attained.
Lack of overhead work
What you end up concluding is the way to solve these types of issues is not to avoid overhead work, but to embrace it. Overhead work enables us to:
- Fully utilize the serratus anterior and trapezius (upward rotators and preventers of winging)
- Stretch the pecs, lats, rhomboids, levator scapula (downward rotators)
- Stretch the infraspinatus and teres minor
This doesn’t mean you immediately start forcing your arm overhead. Some people need to very slowly work on their overhead range of motion. I’ve seen many a people who could only go a couple inches before their pain kicked in, and that’s ok. We don’t push into that pain, and we’ll see the range of motion improve with time.
Forcing me to disagree with this statement from the authors:
“Upon diagnosis, patients should be advised to avoid overhead use of the effected extremity and to avoid activities that cause pain.”
It’s not so much what you do, but how you do it. It’s not so much you shouldn’t bring your arms overhead, it’s how you go about doing it.
You’ll never be able to get your arms vertical by only working them in the horizontal.
–
If you’re looking for some other steps you can take to help with scapular winging, specifically during the day, such as while typing and sitting, you may be interested in this.







{kind=link}
{kind=link}
rightscap
March 11, 2017
Hey! Thank you so much for all of this knowledge.
I’m 20 years old and I’ve had a winged scapula since 5 years back.
During these last 5 years I haven’t been able to bench press or train shoulders.
Pain in right side of neck, my right shoulder is hanging much lower, it feels like it’s kind of loose from my body. But my left side sits perfectly and I have much more developed chest on the left side.
Everything feels so uncomfortable and I used to love the gym.
I’ve been to a three different physiotherapists, one orthopaedic and even got my shoulder x-rayed.
When I read this it kind of hit me, all I’ve been able to do, and got told to do by physiotherapists was to do pull-movements, serratus anterior and rotator cuffs.
I’ve tried so many things under different periods but it never gets better.
But when I try to use my upper traps when lifting my arms overhead it feels easier.
Which maybe means that my upper trap is all fucked up?
My right upper trap is looser and much longer then my left, and everything on the left side sits “higher” and tighter.
Maybe my right side is so “pulled down” and my upper trap is almost dead cause it never gets any work.
I’ve also played a lot of computer and a lot of guitar growing up.
And also, my right internal rotation is very bad. Like this girl on the picture with her arms behind her back.
I’ve decided to try work on my traps, especially upper traps to see what happens.
And to work on serratus anterior.
What do you think of all of this?
And I really wonder what’s a good way to start to train upper traps to get it stronger and tighter?
I’ve searched around a lot of good excercises but I’m kind of confused since I don’t really know how to perform it with a winged scapula/pinching in the shoulder.
Thank you so much for your website, it’s golden!
Take care
reddyb
March 14, 2017
Thank you for the nice words!
Working the upper traps, *in a manner of upward rotation*, is often a good place to start, because that’ll cause the serratus anterior to get work too.
There is this link regarding a progression: https://b-reddy.org/2013/09/05/a-progression-to-lifting-your-arms-overhead-pain-free/
And then if you want more dedicated help: https://b-reddy.org/2013/06/20/the-remote-client-process/
Val
March 15, 2017
I meant to thank you for your response in December and I’m trying to implement controlled overhead movement into my exercise routine. My scapular winging is very weird. My R scapula doesn’t seem to wing with up or downward motion. It wings with forward and side to side motions like when I am pulling my arm back toward me after reaching forward or when I have internally rotated my forearms in front of my body to perform a task like chop vegetables (the bottom tip of the scapula seems to be very mobile) during this task. It will also wing or be unstable when I externally rotate in front of my body as in pulling a piece of paper from an envelope sideways. My shoulder will become weak and seems to lose control while doing any of these tasks. It also fatigues and stiffens when it is propped out to the side while writing on a desk. I developed mod tendinopathy in my supraspinatus and mild tendinopathy in my subscapularis and infraspinatus according to an MRI following my labrum repair in May 2016. All the tendons around my scapula snap and seem very stiff. The more I do with my arm the more pain and stiffness I seem to develop all around my shoulder. My PT still encourages me to do rowing, retraction and external rotation exercises. I would love any further words of wisdom. Thanks again and this website has been very helpful and allowed me to feel less isolated with this big problem.
reddyb
March 17, 2017
Hey Val,
You’re welcome. I cover the internal / external rotation with winging a bit more in this post: https://b-reddy.org/2013/02/12/the-rotator-cuff-is-not-a-muscle/
You want to work on rotating the arm in this fashion, but without letting the winging occur. Can literally stand up, rotate your arm, but practice not letting the scapula wing. While you want to work on this in daily life too, going to be much harder to initially practice this in activities of daily living though, as your mind will be occupied on other things, like not cutting your fingers :).
I’ll have people do this supine sometimes, as the weight of their body on the floor tends to make it so the scapula can’t wing:
Angie
April 21, 2017
I have a 37 year old son who lives in constant pain from a winged scapula and tight rhomboids, LS, and Traps. His arm, shoulder(all the way to the neck) and part of his torso were amputated at age 10 because of cancer. This is getting worse as he is aging. I work on him and the knots come right back. Please help me. What can be done when there is only half a body? Thanks
reddyb
April 23, 2017
Hey Angie,
Sorry to hear about your son’s situation. That’s a very specific situation so it’s hard to tailor advice to it. These are exercises I often use: https://b-reddy.org/2013/09/05/a-progression-to-lifting-your-arms-overhead-pain-free/
Where perhaps the idea of using a surface to push on the scapula can help.
A lot of this depends on the long thoracic nerve. If it was cut or injured in a way influencing the serratus anterior, exercise unfortunately may not work.
On the other side though, the scapula can move independently of the arm. So not having an arm doesn’t necessarily mean a scapula has to be a certain way.
There is a fair amount about winging on this site: https://b-reddy.org/?s=scapular+winging
Not sure if I could give specific help, but I’m always willing to assess first and let a person know if I think I can: https://b-reddy.org/2013/06/20/the-remote-client-process/
Angie
April 23, 2017
Thanks so much for getting back wit me. Let me clarify. The scapula wings on the side that he does have an arm. Sorry , I did not include this.
reddyb
April 25, 2017
Even better! That tends to make it easier. Example of how so here: https://b-reddy.org/2013/12/04/a-quick-way-to-work-on-scapular-winging/
Hampus
May 3, 2017
Hey! I’ve commented and been on this site before. Freaking awesome.
I have had winged scapula about 5 years back, lower hanging right shoulder and so on…
I am from Sweden and I never get this fixed. I am 20 years old now btw.
Is there any way I can send you a video with pictures or something like that ?
To see if you can help me out?
I want to fix this so badly, I love lifiting weights. But I’ve not been able to do it for many years now.
Thanks!
reddyb
May 5, 2017
Hey Hampus,
This is what you want to look at: https://b-reddy.org/2013/06/20/the-remote-client-process/
Brian
Kyle
May 20, 2017
Hi Brian, thanks for the great article. I believe I recently developed serratus anterior paralysis, which I recognize because it happened to me before about 12 years ago. Basically I was having shoulder pain one night and then the next morning had great difficulty lifting my right arm overhead, and when I do clearly my scapula is not stabilized and wings a lot. Also, this came immediately on the heels of a week long viral infection, which I would think is totally unrelated, but from what I read it is actually a documented cause of this type of spontaneous paralysis of thoracic nerve. See this: http://www.oandplibrary.org/op/1964_03_201.asp
I’m glad to read that this sudden paralysis usually resolves itself, and last time it happened it me it resolved itself within a few months with the help of PT. I think in that previous instance the cause was a shoulder injury from Rugby.
Three questions:
1. Can I aid my recover with specific stretches and or exercises?
2. Any recommendations for a sleeping position? Lying down tends to be more painful than normally daily upright positions, which don’t really cause me any pain.
3. Any benefit to wearing a brace for part of the day while recovering and if so any recommendations?
THANK YOU SO MUCH!
b-reddy
May 23, 2017
Hey Kyle,
Thank you for the nice words.
-Wow, I’ve never heard or would have thought of serratus anterior paralysis due to a viral infection. That’s pretty wild.
-I go over some exercises in this post- https://b-reddy.org/2013/09/05/a-progression-to-lifting-your-arms-overhead-pain-free/
(If you want to get more specific to your situation, you may be interested in this: https://b-reddy.org/2013/06/20/the-remote-client-process/ )
I go over sitting position and winging in this manual as well: https://b-reddy.org/2015/07/20/why-typing-annoys-your-neck-shoulders-elbows-and-wrists-and-what-to-do-about-it/
-Laying down and you want to lay on your back as much as possible. When on your back, provided the mattress isn’t super soft, you have the force of your body meeting the force of the bed, with your shoulder blade in between. Where the shoulder blade gets pushed into the ribcage, a good thing! (You’ll see many of the exercises in the link above involve the floor or a wall, helping prevent winging.)
When laying on the side, particularly on the side that’s problematic, winging is more likely. Been meaning to write a post with some pictures of this but haven’t gotten to it yet.
-I’m not a big brace guy. It’s not that I don’t think people can find it helpful, but besides often being expensive and potential trouble in getting the right fit, my fear is a person doesn’t learn to correct the issue volitionally. That once the brace comes off, the issue can easily come right back. It’s sort of like crash dieting. At some point, a person can’t keep that up. Because they never truly learned to change their habits, they fall back into their overeating and the weight comes back.
Bastien
August 21, 2017
Hello Mr Reddy, Quick question :
Does the subscap will be trained enough when doing overhead work ?
Humeral depressor is part of its feature, but we don’t work “the internal rotation feature here”.
For someone (like me) with tights infraspinatus, is it better to lift overhead with a pronated grip than a neutral grip ?
I always think it was safer for my shoulder to lift with a neutral grip but I think its a wrong thinking because I’m don’t stretch enough the infraspinatus/teres minor while doing so (because my humerus is not in internal rotation …)
Do you agree with that statement ?
Your blog is very informative,
Regards,
Bastien
b-reddy
August 22, 2017
Hey Bastien,
I don’t like relying solely on overhead work if the subscapularis clearly needs work. I’m big on shoulder rotations.
Supine: https://www.youtube.com/watch?v=Yr9W20OcTZk
Standing: https://www.youtube.com/watch?v=iYZvba2M4no
With a good focus on the humeral head never translating forward or upward. That is, it only rotates.
When it comes to overhead motion, I’m not sure I’ve ever seen someone with tight external rotators. For instance, where the elbows turn *in*. (Elbows turn out => internal rotation; quite common.) I’ve seen this manifest with the shoulder rotations per above, but not in overhead motion.
Raising the arms with purposeful internal rotation is not something I’ve done, and something I’d be cautious with. It’s actually a provocative test for shoulder impingement. If tight external rotators are a problem, I’ve always been able to assess and correct it with the shoulder rotation exercises.
Thank you for the nice words.
Bastien
August 22, 2017
Thank you for your answer.
Actually I don’t feel tightness at all in my infraspinatus / teres during overhead motion BUT like in your article, I have a winging scapula when I place my hand behind my back (like the woman in the picture above), so my external rotators (the rotator cuff ones) are too tight I think.
That’s why I asked you if the subscap will work “enough” while doing overhead work.
Anyway you did answer to this question.
So I do need some subscap strengthening to improve my internal rotation and be able to scrap my back more easily (as my external rotators will be stretched). I will do your recommendation (standing internal rotation seems good to me 🙂 )
Note : my main goal is to get back some flexibility as I had surgery in December 2016 (Distal clavicle resection for my right shoulder) and my internal rotation is the last thing that I struggle with ..
Best regards,
(Sorry if it was not clear, my English is not perfect …)
b-reddy
August 25, 2017
Hey Bastien,
About to respond to your email.
Daniel Deitz
October 24, 2017
Hey, im a baseball pitcher and over the summer I just tightened everything and wasnt strengthening like i should. I can tell i have a wing in my right scapula, and also i can tell my right shoulder sits lower. Thus article cleared alot of things up. The only question I have is why do alot of people say to stretch the traps and strengthen the adductor like the rhomboids? Im just confused because you say to work the traps and reteach them how to fire and to stretch the rhomboids. If the rhomboids are meant to pu the scapula together wpuldnt atretching them not help the issue? I just want aome clarity so i can do the right thing and fix this issue
b-reddy
February 6, 2018
Hey Daniel,
Sorry for the delay. I had a technical issue where I missed some comments.
In the post I mention the rhomboids can be part of winging, but it’s rare. So they don’t typically need attention, whereas the serratus anterior does. Which is important because the serratus anterior (upward rotation) does the opposite of the rhomboids (downward rotation).
As far as why so many focus on the rhomboids, such as phrases like “pull your shoulders down and back,” I have an article coming about that. Tough to clarify in a comment. In brief, many have mistaken excessive scapular anterior tilt for excessive scapular abduction. What people have really been trying to say by “shoulders back” is “shoulders posteriorly tilt.” We want the shoulders to *tilt* backwards, but not be pulled together backwards.
Corey
August 5, 2018
Hi Brian. Amazing post and makes it easy for people to understand what’s going on with the scapula.
I tried doing the standing shoulder rotations and i get a huge pinching sensation in both shoulders at the top. (Only one shoulder has the scapula winging/pain.)
Just wondering if you think its impingement? ( even though i have done many online tests to test for it and came up negative such as internally rotating the arm and crossing arm over the body ) which doesnt hurt at all.
Also i went to a osteopath and he said my sub scapularis is not working properly.
Could this be related to my winging? (Only on right side)
b-reddy
August 7, 2018
Hey Corey,
That’s tough to say without seeing the motion. These might be helpful though:
https://b-reddy.org/demonstration-of-humeral-superior-glide-with-animation-and-voiceover/
Superior glide is more commonly associated with classic impingement.
Anterior glide can cause impingement, but you’re talking more the biceps tendon in that case.
Winging isn’t so much the problem with this motion as is anterior tilt, though they can happen simultaneously.
Michael
December 18, 2018
Hi Brian. Wonder if you have enountered with my kind of issue with winging.
My main concern is pain in lower trap unilaterally. It definetely overworks for my serratus, but upper trap is relatively strong, so I find myself in constant upper rotation and anterior tilting. Lower trap fires in all movements of upward rotation, posterior tilting and retraction. In one post you prompted to use small amount of arm flexion for posterior tilting, but I can’t use it, because my lower trap immeditely fires, resulting in pain (but, yes, no winging) (https://b-reddy.org/a-quick-way-to-work-on-scapular-winging/) I also have forward shoulder, tight pec minor and rotator cuff.
I am trying to exercise it out, so have a few questions: how could it be better to train serratus, not firing lower trap? For example, in wall slides should I prevent scapula depression and retraction (coolig down lower trap), even though it leads to excessive shoulder protraction?
In the end, you have a really gorgeous site, definetely one of the best that I have ever come across. Cheers from Russia,
Michael
b-reddy
December 21, 2018
Hey Michael,
Thank you for the nice words.
Pain around the inside of the scapula is common with winging.
Having too much upward rotation is quite rare. To where I’d want to assess you before being ok with that conclusion. What you may be thinking is too much upward rotation could be too much abduction i.e. the scapula is too far from the spine. Those people can have discomfort / pain at rest, to where you just retract their shoulder blade a little, and they often start feeling better. This is also rare (too much retraction is more common), but it happens.
When it comes to exercising, I’m not sure I’ve ever worried about someone working their lower trap too much. As you hit on, lack of posterior tilt is common, to where working the lower trap helps.
If you’re having that much issue with exercise, there are two things you probably want to do-
1. Not worry much about exercise until you get your daily activities to where the shoulder area calms down
2. Significantly regress your exercise routine
Saying 1. another way- sometimes a person can’t really do any exercise until they get daily life feeling and working better.
Lastly, while knowing muscles helps, I’d largely look at it from a movement perspective. As you can see, when you try to break it down muscularly, it gets very hard. Rather than say, try to work upward rotation while not working the lower trap much, I’d instead work upward rotation and limit any painful or abnormal movement that may be occurring (if any) during the motion. The muscles will work themselves out if the movement happens the way you want it.
(Again, that assumes you can or should be working on that with exercise, rather than only focusing on ADLs right now.)
Sorry if that’s a bit vague, but this does sound more like a client assessment scenario. (If interested: https://b-reddy.org/the-remote-client-process/ )
Jonny Wang
April 6, 2020
When leaning on the elbows the humerus can become displaced anteriorly (forward) and or superiorly (upward), lengthening the subscapularis.never thought this muscle could be stretched by this movements (sup,ant) only thing i knew was to lateraly rotate it iam trying to learn anatomy but there is not such information i am confused. why anterior or superior movement can stretch sub
b-reddy
April 7, 2020
In my experience seeing people learn anatomy, the common approach is to memorize where a muscle is, and what a textbook’s definition of action is.
Doing solely that can make it pretty arduous as you’re just playing a regurgitation game.
For me, what really brings it home is looking at the orientation of the muscle fibers and visualizing how they work. In many cases, you can understand the muscle’s action(s) just by looking at where it is and how the fibers are aligned.
Greg M
July 24, 2021
I think your almost 100% correct.
I didn’t read absolutely every line in this article, this the almost part…..😅
However as I suffer from the same winging as what was shown, I know your right.