I’m cruising around the American Journal of Sports Medicine one day and I come across this paper:
Because the AJSM always requires you to pay to read their stuff, to the tune of $36 for this one article, I read the abstract.
“For males, a model that included ACL volume and the lateral compartment posterior meniscus to subchondral bone wedge angle was most highly associated with risk of ACL injury, where a 0.1 cm3 decrease in ACL volume (approximately 8% of the mean value) and a degree decrease in meniscus wedge angle were independently associated with a 43% and 23% increase in risk, correspondingly.”
I had never heard the term “meniscus wedge angle” before. I gave it some thought, reread the abstract, and thought, “well, that makes sense.”
As I said, I can’t access the full paper for this. (I rarely pay for research like this, for reasons I’m sure I’ll write about another day.) I have to do some guessing, but I think I get what the authors are aiming for here.
What’s a meniscus wedge angle?
There is virtually nothing on this out there. From what I can tell, this may very well be a term the authors of this paper made up. For instance, type “meniscus wedge angle” in google and this paper is the third response already, and it’s from 2015. (That’s a high ranking for a new, non-news page.) I also asked an orthopedic surgeon if they’d heard of this term, and they hadn’t. So it doesn’t appear much has been written on this previously. That doesn’t mean it’s insignificant. I mean they may have found making up the term to be more appropriate than any other terminology out there.
What I think they’re going for here is this:


–
Why would this angle matter?
If we use a wedge to block the back of some car tires, to prevent the car from sliding down a hill, we pick the bigger wedge over a smaller one. The taller one.


Note this is a rough analogy. Menisci are mobile. They can move around some, where a wedge with a car (hopefully) cannot.
This makes perfect sense as to what you would (probably) want in a knee- big wedges around it, predominantly on the sides, to help prevent too much (side to side) movement. What happens when the knee moves too much? Like this?

You injure your knee. Torn meniscus, torn ACL, maybe some others, but those are the two big ones.
Smaller wedges and the knee bones can more easily move-

Bigger wedges and the knee bones can’t as easily move-

Shallower falls out of the boundary, while the deeper does not:


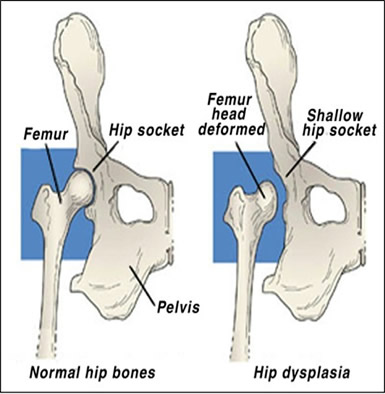
The other way to think of this is these wedges can provide a deeper joint, which is a more stable joint. We know this with the hip. Hip dysplasia is where the hip joint is too shallow, making it much more easy for the femoral head to slip out of the acetabulum.


Notice the femoral heads falling out of the acetabulum / hip socket. (This is a dog, and that’s its tail, by the way. (From: http://www.expertvet.com/sites/default/files/Hip%20dysplasia%20-%20PVSEC%2011-2013.jpg ).)
Shallow joints are not the best friend of someone who needs stable joints.
” a degree decrease in meniscus wedge angle [was] associated with a…23% increase in risk [of ACL tear]”
Because abstracts always like to use relative risk to make their results seem more than they are, I’m assuming that’s what’s going on here. Meaning I don’t know what the absolute risk these authors are using as their baseline. For instance, for the population we’re looking at,
- Say 1 out of 100,000 tear their ACL. That’s 0.00001.
- Let’s say an increased risk of 23% translates to 23% more ACL tears = 0.00001299.
Then that’s not exactly a big deal. The absolute number is still so low. Actual ACL numbers seem to be around 200,000 per year. (This is injuries; not surgeries.) The population of America is 320 million.
- 200,000 / 320,000,000 = 0.00065
- Increased by 23% = 0.0008
However, if we decrease the meniscal wedge angle by four degrees, we’re getting to where the risk can be ~doubled (100% increase).
- Doubling 0.00065 = 0.0013
Again, still may not be big in terms of absolute numbers; few are to where they tear their ACL simply by walking around, but it’s likely not something you want. (In terms of the general population though, that’d be an extra 200,000 ACL injuries every year!)
Once we start looking at this in the context of dynamic activity, like athletes, I can see this stuff starting to matter. Again, not to where you run out on the court and you bam, tear your ACL. There are some out there who seem so prone to these types of injuries though. Those who, once put in a certain context, injure their knee(s) seemingly every X amount of months. Some athletes out there who are on their third ACL surgery. Some with multiple knee surgeries before high school ends.
And then many of us have seen the person who was completely fine, running around, then out of nowhere hits the ground. Nobody touched them, nothing unusual happened. Their knee merely gave out.
-> To be clear here, I’m not suggesting a meniscal wedge angle by itself accounts for the above type of person. I’m saying it could very well be one of many factors. Where, when you add all these factors up, you get quite an increase in odds of tearing the anterior cruciate ligament.
This is also where we can get into why some have such a hard time coming back from certain knee injuries. They may have some predisposing factors which not only made them more likely to have the injury, but harder for them to come back. A knee with decreased wedges already has lesser stability. It sure as hell ain’t helpful to have that.
This is where I think these types of factors, things which are really not too well understood, come into play. Things that may very well be 100%, or close to it, genetically based.
-> This also gives us some semblance of what “it’s genetic” actually means. I’ve had some ask me about genetic factors with knee injuries. This all could be a “genetic factor.” But now we have a specific meaning for that, which means we can derive some practical application.
Lastly, this is only one factor. This group of researchers have looked at some others, which I may delve into in other posts. Things like how thick the ACL is, the orientation of the knee bones, and more. It makes sense the more of these risk factors you have, the greater the increased risk of ACL injury.
There are a lot of things out there about ACL prevention. Things like strengthen the hamstrings, be strong in general, proprioception, working on landing, and it’s all worthwhile stuff. But it’s worth knowing some of us may not have joints made for certain sports. Hard work cannot always beat talent, especially when you may not even know what you’re not talented at. Sometimes it’s obvious. You watch someone high jump and they gracefully bend their spine over the bar. They don’t have to work to achieve that level of mobility; they just have it. Meanwhile, you try, and this happens:

HT: FunnyOrDie
However, sometimes it’s not initially obvious. Sometimes you’re on your second ACL tear by 16 years old, and hopefully someone around you goes, “Look, you’re not made for X.” (Below I give some ways to potentially draw this out sooner. Maybe before such a terrible injury happens.)
-> This stuff isn’t exactly worth bragging about either. The athletic world is notorious for calling people soft because of how often a certain player may get injured. These types of psychological attacks may very well be analogous to calling someone a pussy because they and their red hair don’t handle the sun well. Or bragging how well you handle the sun because of your tan skinned heritage. It’s not like you earned that, or worked for it. It was given to you. On the flip side, it’s not your fault if you don’t have this. No. Really. It’s not your fault.

–
A silver lining and practical applications
I’ve written about this type of stuff with the hip before. (Here, here and here.) One thing I delved into was one should not always feel discouraged by these limitations. That while you may not have as much of something as another, perhaps joint stability in this case, you may have more of something than another, joint laxity in this case. Whenever you gain something, you lose something.
Let’s think about the shoulder. If you’re an American football player, the last thing you want is a congenitally lax shoulder. The shoulder is something you’ll have to land on a lot, like with tackling. It’s something that will have to withstand a ton of trauma. You don’t want it popping out every time you hit the ground, or in any way more susceptible to that happening. What if you’re a baseball player though? What if you want to do this?

Humeral retroversion.
(A quarterback may apply here as well. Although the arm demands aren’t as severe at QB, compared to pitcher.)
You want a very lax shoulder then. And what do you find with baseball pitchers? Many of them are very lax. Some are so lax you can see what is called a positive sulcus sign i.e. you can manually dislocate the shoulder pretty damn easily!
Light example-
–
Extreme example-
–
-> 61% of professional pitchers have been found to have this, with 89% of those having it bilaterally. Indicating a solid argument it’s genetic; not developmental. (Also indicates you don’t have to have this trait to be a professional.)
Making an argument for a lax knee: Perhaps in ballet it’s advantageous. When you’re trying to get your knee to turn like this,

You don’t want wedges which block too much side to side movement. You’d want tire(s) to not be as stable.
-> Remember talking about hip dysplasia earlier? How hips which so easily fall out of the socket are not very stable? What are they though? Incredibly mobile. What population do you find with incredibly mobile hips? Dancers…89% of dancers have been found to have borderline to full hip dysplasia! That’s not a hip you’d want to be playing basketball on, but if you need to get your foot to your head?
Ironically, pitchers also do this a lot with their push-off leg.

Notice the bottom portion of the leg turned significantly out from the knee. The foot is turned sideways of the knee. The knee is nearly pointing towards the ground, while the foot hasn’t made it there yet.

You can also see some side to side motion on the landing leg:


-> I think this is where a lot of the notion of pitchers shouldn’t lift weights has come from. Good pitchers tend to be very lax people. Guys who excel at lifting weights tend to not be. So the thinking has gone -> Those who want to be good at throwing -> Shouldn’t lift. It will make them “bulky” and stiff. But this is really congenital stuff we’re talking about here. In other words, a pitcher with a positive sulcus sign is unlikely to significantly lose that from lifting. Plus, these types of athletes are already good at the flexibility part. If anything, you probably want to be giving them stability, to help with injury prevention. And the last thing you need to do with these types is stretch them even more.
Continuing the theorizing: Say you have the same amount of meniscus volume, but you get to decide where it goes. We have our wedges as one example-

But we could also move that volume around, so our meniscus is more horizontal-

The wedge angle is less, but the meniscus’ thickness is more evenly displaced.
This knee may not be great from a side to side stability perspective, but it may have a laxity benefit. Furthermore, I could see this knee handling forward and back movement -that is walking or running in a straight line- very well.

It has extra cushion between the knee bones. More of the meniscus is getting loaded in this case; lessening the loading on other areas. Perhaps this is something marathoners have a propensity for, and it’s what enables their knees to handle extreme workloads. Anecdotally, long distance runners are usually good and only have been good at one sport- long distance running. I’m not sure I’ve heard a top distance runner go “I was good at basketball and football too, but decided to concentrate on marathons.” Perhaps they don’t have the joints for many other sports, like those involving cutting back and forth.
As I said, it’s unlikely we get to pick what category we fall into. There may be some room to train yourself into another category (discussed this with the hip), but you probably have to start very young.
-> This is similar to throwing. If you don’t start throwing young, it’s very hard to acquire a throwing range of motion later in life. Those who “throw like a girl” do so because they never threw growing up.
I will say that if you’re someone who has always had a proclivity for throwing a ball, you probably fit into the genetically flexible world. If you’re someone saying, “I think I’m this way, but I want it that way,” I submit to you this:
–
-> Another observation here: It’s been well documented those with a more recent departure from Africa -what we call African Americans- dominate certain sports. Running events in track, American football, basketball. One area I don’t believe this dominance has extended to though is anything involving throwing or things throwing oriented. If anything, white people -those with a less recent departure from Africa- seem to excel at that. Volleyball, softball, baseball, quarterback in football, tennis, golf, swimming, throwing events in track. (Hockey too, which, while not throwing oriented, can require a ton of mobility.) I’ve covered some of the reasons for the black dominance in certain sports, I wonder if congenital laxity is part of the dominance for whites in others.
-> Again, this is a spectrum of dominance. It’s not that one race exclusively dominates one sport. (some) White people can jump- the highest vertical in the NBA combine this year was a white dude from Notre Dame. On the other side, African Americans can still do well at tennis. Serena Williams has done alright for herself.
–
Giving kids the best chance for sporting success
A quote that has stuck with me from one of my client’s was, in reference to his own son playing sports,
“There’s no point in sticking with something you’re only going to be endlessly frustrated with.”
This particular person’s son was having a tough time excelling at things running oriented. Soccer for instance. The dad eventually convinced the son to try something more cerebral, which he excelled at. They picked up golf (happens to be mobility based!), and the son ended up being good enough to play in college.
Now these types of things are very hard to predict, but I think it may be worth exploring the notion that if your son or daughter is gifted at things which require a good deal of mobility, the sports I listed above like swimming, throwing oriented ones, hockey, then it may be a solid idea to steer away from sports which don’t embrace mobility. If your kid is good at pitching, linebacker / football may not be the best fall sport. (If nothing else, that valuable arm will get beat up!) If your kid is a great swimmer, they probably won’t do great as a sprinter. Flipping things around, if a kid is good at rugby, ballet may not be a good offseason workout. Or at least one you’d want to be careful with.
Not only will they likely not be great at these sports, but what I’m getting at here is a good pitcher may -due to what makes them good at pitching- be more likely to get hurt as say, a soccer player.
–
If I worked for a professional sports team…
Using the NFL as an example- With how much money is invested in players, and how much money NFL teams have, something like MRIing every draft picks knee you’re interested in may not be out of the question. Or at least certain picks, to where you analyze these types of risk factors. (This is already done to some degree.)
If they only have one risk factor, like smaller meniscal wedges, then maybe you don’t read much into it. However, if you need a tie breaker between two draft picks, this could conceivably be one. An objective one! Nobody’s opinion needs to be accounted for.
If they have a huge discrepancy, and or multiple factors, then this could be the difference in drafting them or not.
Or if the player already had a knee injury, and they have these factors, this may scare you away from drafting them. (Barring quarterback, I would never draft a player fresh off an ACL surgery though. Unfortunate, but reality.)
You could also use this stuff in free agency, or with a player who has been recently injured and whether you want to release them and move on or not.
As evidenced by the fact the NFL’s average turnover for players is 3.5 years, there are practically an endless supply of players out there. There are very few who teams truly fall in love with. Things of this nature could prove to be difference makers in the decision making process, and huge money savers. At the top of the wish-list for every coach in every league is Staying Healthy. This may be where a next barrage of “sabremetrics” could come into play.
For 2014, let’s say there were 62 ACL injuries in the NFL. 62 ACL tears per calendar year, not only in season. (This is likely, if anything, a bit low.)
- 62 injuries / 32 teams = 2 injuries per year per team
- An increased amount of 23% would be 77 injuries per 12 months.
- A doubling would be 124 injuries per 12 months
- 124 ACL injuries / 32 teams = 4 injuries per year per team
When your roster is 53 guys, going from losing 2 to 4 guys each season represents going from losing 4% to 8% of your roster. 8% of the 2015 salary cap (133 million) is about $10.5 million. When you’re starting at only 2 guys per year, there may not be much room for reduction, but there is a lot of room for increasing. Looking at these factors could conceivably help a team avoid this.
Or let’s say you derive a model of multiple risk factors, and you find by accounting for all those factors, you can decrease the amount of ACL injuries on your team by one person per year.
- 1/53 = 2% of your roster
- 2% of your salary cap = $2.66 million
Not much, but this is only one year. Do this over say, 10 years, and you’ve just saved yourself 26.6 million dollars. Even if you only decrease the amount of ACL injuries by one every other year, that’s $13.3 million.
Not only that, but you don’t have to pay someone else to take the injured person’s spot, while you pay the one guy during his rehab. An ACL injury often takes a full year to recover. So we have a full year of paying one guy’s salary to not play, and paying another guy’s salary to play.
- $2.66 * 2 = $5.32 million.
- Or $53.2 million over ten years.
- Or if only every other year, then it’s $26.6 million.
Getting these savings could likely happen for a minimal investment.
Let’s say every team chipped in to MRI every NFL combine member each year. On average it seems there are about 300 players at each combine. The last MRI I paid for, I paid in cash. Partially because I have a high deductible; partially because I wanted to know how much they actually cost. (Tell the imaging company you’re paying cash and you’ll finally know much it actually costs.) I paid $400.
- 300 players * $400 = $120,000
- $120,000 / 32 teams = $3,750 per team
$3,750 spent per year, helping you save $5.32 million? Or $2.66 million? Not bad!
And we haven’t even accounted for the financial impact of losing a guy on your roster beyond the salary cap. If you lose a starting player for an entire season, the financial impact could be much higher. The season Tom Brady tore his ACL the Patriots didn’t make the playoffs. Quite a rarity for New England. What’s the financial impact of that? Or of winning one less game? Or having an exciting player on the sideline?








{kind=link}
{kind=link}
{kind=link}
{kind=link}
Posted on September 14, 2015