I recently visited the Washington University in St. Louis for the second time. The first time, close to two years ago, was for help coming off my ACL reconstruction. (There is always something to be said for having someone’s else’s eyes. They will see things you can’t.) This time was to attend one of their Movement System Impairment courses. The first time was to help me get looked at, the second time was to help me look at others.
They have a few different courses. I went with their most general / introductory one. Primarily because I had to. In order to go to their advanced courses you have to go to the general one first.
The course is two days, a Saturday and Sunday, and ended up being about 18 hours of lecture, watching assessments, assessing others, getting assessed yourself, and asking questions on the side. It was nine hours straight each day of my mind being so focused I think I almost understand what coming down from a cocaine high is like. I literally had a headache after each day. There were plenty of breaks, but I ended up using those as opportunities to talk to the therapists on the side.
Another impetus for me attending this was Shirley Sahrmann was speaking. Shirley is I believe 78 years old, and professor emerita. “Emerita” is supposed to mean a retired professor, but nobody seems to know exactly what it means. Point is, it seems she’s towards the end of her career, and I’ve been worried I may miss out on ever seeing her in person. When I visited in 2012 I tried emailing her to no avail (which I joked with her about); ending up with a different therapist. In going to this course I was guaranteed to at least see her speak.
And speak she did. I was thinking she might do the intro then let the other faculty take things over. Shirley spoke for about eight hours on Saturday, and was in some shape or form part of Sunday for around six of the nine hours. (See what I mean about “retired” professor?) I also talked to her for about 15 minutes one on one, which I did not expect. She was hysterical, sharp as hell, and as informative as you’d imagine somebody with 55 years experience and her brain power to be. She is scheduled to speak in multiple events this year. I highly recommend seeing her if you haven’t already.
Much like my visit to Stanford, there is going to be a lot in this. I’ve posted a good deal of this in specific posts already (on the homepage), but there are some sections original to this post. You can click the following links to be taken to the specific sections on this page.
- What’s moving too much?
- “Arthritis is a normal response to abnormal stimuli”
- “You get what you train”
- “You can stop working on how you move when you stop moving”
- “If we studied normal gait now, we’d have to revise everything”
- Oddities in knee alignment
- A short muscle doesn’t equal a long muscle
- Some amazing new surgery, or a sign of the times?
- My conversations with Shirley
- Getting shorter with age: It’s not just the spine (why your pants are longer now)
–
What’s moving too much?
Shirley referenced someone who started to have back pain after a knee replacement.
“Why do you think their back started to hurt?
…
Because their back became more flexible than their knee.”
And we have the concept of relative flexibility. How much is everything moving in relation to everything else? In the above example, how much is the knee moving relative to the back?
Envision someone who’s had knee surgery. How much can they move their leg immediately afterwards? Not much. So, how do they do things? How do you pick something up? How do you reach for something? How do you do all these things when you can’t use your legs as much? You have to get the motion somehow. That somehow is usually by moving the lower back more than it would normally move. You can’t bend your knee(s) to help you pick something up, so you bend your spine instead. The spine becomes more flexible relative to the knee, which can become more stiff.
Furthermore, the lower back is moving more than it normally would. This is where the pain comes in. The prevailing theme of this approach is what moves too much, hurts. Shirley repeatedly states, “I don’t care how much you don’t move.”
You find what moves too much, you find what direction it moves too much (anterior, posterior, rotation, etc.), you find when it moves too much; you stop all these things from happening, and the person usually feels better.
This is a paradigm shift for most, as most have spent forever trying to figure out, “What do I need to make move more?”
The shift is 1) You don’t always need to make something move more. There are some who are congenitally lax, people with just crazy flexibility everywhere, who still get in pain. Flexibility isn’t their problem, relative flexibility is. 2) You can try to make something move more, but you damn well better be simultaneously trying to make something move less. After a knee replacement you can’t only worry about trying to make the knee move more, because you often end up compensating by moving the lower back more. (See here.) You have to make the knee move more while making sure to move the lower back less / not at all.
–
Back to Top
“Arthritis is a normal response to abnormal stimuli”
Your knee has been hurting a while. You get some X-Rays; the doctor comes back and states you have pain due to osteoarthritis.
This statement by Shirley: “Arthritis is a normal response to an abnormal stimulus,” is saying something profoundly different. You have arthritis in your knee due to something else. That something else? How you’re moving.
Say you had a meniscal tear in your right knee. Because of this tear you have some instability. Or, you suffered the tear because of instability. Either way, you have issues at your knee.
In the context of the “movement system,” instability means your knee is moving too much in a particular direction. It’s hypermobile. Like someone whose knee caves in too much, too often. The body doesn’t like this. It’s equilibrium has been thrown off. What does it do? It tries to stabilize things of course. How can it do this? Arthritis.
What’s one way to block movement? Put some bone in front of it. What does arthritis do? Lay down extra bone. The body uses arthritis as a method to hopefully change how the knee is moving. It’s trying to make the knee LESS mobile. This is a reversal of conventional medicine, which tells us “You have arthritis, now you have pain.” Shirley’s statement is saying, “You had some issue before, now you have arthritis.” This is crucial because it dictates the treatment. You don’t go trying to get rid of the arthritis in the hopes that solves the issue. [1] You solve the issue in the hopes your body stops needing to generate arthritis!
Another example: If someone has lower back pain long enough what happens? The disc(s) atrophy, then the body lays down bone, such as spurs, and eventually the spine may fuse. Where does it fuse? At exactly the location the person is moving too much!
The body knows what’s wrong. If you don’t correct things by changing how you move, the body will eventually force you to move differently. It’s like when people drink too much. If you don’t stop drinking, the body will make you. It will make you black out, it will make you pass out, it will make you vomit, it will make you feel like a bomb went off in your head, it will make you forever hate the smell of a certain type of liquor, whatever it has to do in the hopes you’ll adjust your drinking. It’s trying to help you. It’s trying to make sure you don’t poison and kill yourself.
More specifically: If you don’t stabilize your spine, your body will do it for you. This is why you rarely see people with lower back pain their entire lives. At some point it goes away because the body will handle things on its own.
It’s so rare the body doesn’t have a legitimate reason for what it’s doing. We all know the 10 year old who gets cancer with no apparent explanation, but this is the (extreme) outlier. The body doesn’t just do crap to hurt you. It doesn’t just lay down new bone to piss you off. It’s doing it for a reason. A reason almost always to your benefit.
Stop saying “Your body is a piece of shit,” “My body sucks,” “My body hates me.” It’s telling you something. You need to figure out what. The body is doing its part; you need to do yours. I’d wager in even the extreme outliers, the body is doing something for our benefit, we just don’t know how or why. [2]
Is the body always right? Is it always doing things perfectly? Of course not. But people say with age you gain wisdom. Think about how long the human body has been around, how much it’s gone through, how much it’s seen…It has quite a bit of wisdom.
–
Back to Top
“You get what you train”
One of the other tenets of the Washington University philosophy is you get good at what you regularly do.
-Lean on your arm a lot? You get good at leaning on your arm.
-Turn your knees in often? You get good at turning your knees in.
-Sit hunched over? You get good at hunching over.
The sitting hunched over is a poignant example. It’s not only you hunch over a good amount while sitting; it’s you hunch over a good amount while sitting, and because you sit 10 hours a day, your body gets good at hunching over all the time. So, not only do you hunch over when you’re typing, you probably hunch over when driving and when standing too. “You get what you train.”
Or, what I also like to refer to as, “Whatever you regularly do, is what you regularly do.”
Fancy, I know.
Shirley gave a couple other unusual examples that really drive home this point. First, she mentioned you can notice extreme endurance athletes will sweat a good amount even during a relaxed physical therapy examination. Why? They’ve trained themselves to be really good sweaters. Second, she’s noticed recently, especially with males, a propensity to tense their muscles as soon as she touches them. After prying she discovered this was due to the MMA athletes she was seeing. What do MMA guys do as soon as someone touches them? Tense the hell out of their body to prevent their opponent from doing what they want.
–
Back to Top
“You can stop working on how you move when you stop moving”
I cracked up at this one because this is something I run into way more than I ever thought I would.
One of the more common setbacks people have is once they start feeling better, they start slacking off and their old habits come back. No big deal. We all do this. Myself included. You get back on the wagon and keep moving forward.
What many struggle with is you are forever on the wagon now. You might fall off sometimes, but you’re never getting off for good again. At least you’re not supposed to.
For example, a person has shoulder pain. They start doing some exercises designed to help with their shoulder, along with modifying how they do certain things during the day. Like how they type. After a few weeks of feeling better it’s common to think, and it might be subconsciously, “Eh, I don’t need to be as diligent with that stuff anymore. My arm feels a ton better.” Some people will get away with this. For many, slowly the pain starts coming back.
Again, there’s no judgment here. None of us want to do more work than we have to. As Seinfeld has joked, “Anything requiring more than me laying in bed is work.” Exercising, being cognizant of how you type, is work. Work that can become habit, but old habits die very hard indeed. In fact, we’re learning some habits may never actually die. Like riding a bike, the brain doesn’t forget certain things.
What’s difficult to grasp for some is the fact they will have to work at keeping their arm healthy the rest of their life. As long as their arm is moving, they need to work on how that arm moves. People think they can do their exercises for a month, then they’re forever cured. Doesn’t work that way.
When someone gives up smoking they don’t think, “Alright, I’m going to stop for a month, then I can go back to a pack a day.” They don’t even think, “Alright, I’m going to stop for a year, then I’ll start up again.” No, the health issues are going to come right back.
Ask anyone who was a smoker for a long time and then quit for a long time. They’ll tell you they still get cravings. It might not be as bad as it once was, but it’s still something they have to work on.
Exercise, and HOW you exercise (move) are no different. In the beginning, it takes a lot of work to get off your ass and do it. It can take even more work to really pay attention to how you’re doing it. (One reason to hire someone. They do the thinking for you.) Over time, it’ll get easier. But, it’ll never be something you don’t have to pay attention to. And sure, you might have a cigarette here or there. But you can never again be oblivious. If you are, the cigarette here or there will slowly become the pack a day again.
When you’re not feeling like working, try to flip things in your mind. Be thankful you actually know what to do to correct the issue(s) you have. While it might be a pain in the ass you have to do a few things regularly to not be in shoulder pain, think of how many people don’t have that option. They have to be in pain because they don’t know what to do.
–
Back to Top
“If we studied normal gait now, we’d have to revise everything”
Robert Sapolsky has a great lecture series called Being Human: Life Lessons from the Frontiers of Science. He tells the story of treating Sudden Infant Death Syndrome (SIDS).
For a long time SIDS had no understandable cause. Eventually, in the early 1900s, we delved into this disease and examined a bunch of SIDS cadavers. This was a great opportunity as cadavers represent one of our best diagnostic tools, especially a hundred years ago. We can look inside the body and go, “This group, who died of this disease, seems to have this commonality.”
Upon opening the SIDS cadavers we found an obvious congruity. All the SIDS babies had enlarged thymus glands. Understanding their death became easy: Too enlarged of a thymus gland could asphyxiate the infant, causing quick death.
We immediately formed a solution: Irradiate the thymus gland, causing it to atrophy, and boom, no risk of suffocation.
The result? Ten thousand people were killed, and many more harmed.
“Wait, what?”
To understand this you need to consider what cadavers were looked at, and their relationship to what we considered “normal” bodies at the time.
In human history, through a myriad of mechanisms, the majority of cadavers have been from poor people. Executed criminals -who are usually poor- often had their bodies donated to medicine. Bodies were even stolen from graves and sold to medical schools. What bodies were easiest to dig up? What bodies were least likely to have solid coffins? Poor people’s.
So, we’re at the early 1900s, and nearly all the cadavers we’ve studied at this point are from the poor.
We, especially in the United States, often assume more money is always better. In more recent history, one of the revelations when it comes to the relationship between financial well being and physical well being, is a plethora of money doesn’t lead to a plethora of health. But a deficiency in money can lead to a deficiency in health. Being rich isn’t healthier than being middle class, but being middle class is way better than being poor.
In the States the median household income is about $50,000. The median household isn’t going to add much to its health by striving for more income. It can hurt its health by not staying at this level though. As Sapolsky states, some of the best health advice is, “Don’t be poor.”
One of the obvious health issues with being poor is the strain that accompanies trying to make ends meat. The constant stress hurts the immune system. What’s a gland with a big role in immune function? The thymus. When you’re chronically stressed the immune system never gets to work like it should. What happens when something in the body doesn’t get to work like it should? It atrophies.
Poor people => Chronically stressed => Atrophied thymus gland.
So, we’re at the early 1900s, and nearly all the cadavers we’ve studied are from the poor with atrophied thymus glands.
By the definition of SIDS, the death is sudden and unexpected. In order for a death to be such, the infant must have been healthy beforehand. What infants are most likely to be healthy? Certainly not the poor.
What happens when you get a bunch of SIDS cadavers? You get a bunch of cadavers who are not similar to what’s been studied so far.
Cadavers of poor infants => More likely to have atrophied thymus glands.
Cadavers of SIDS infants => More likely to have regular sized thymus glands.
But, when you’re idea of normal is smaller than it should be, what do the SIDS thymus glands appear as? Too big. Doctors studying the SIDS cadavers go, “Ah ha! These thymus glands are all too large. If we can make them smaller, we can prevent SIDS!”
Doctors began irradiating normal thymus glands thinking they were all bigger than they should be. Their idea of normal was skewed. When you irradiate a bunch of regular thymus glands and the organs around it, you end up predisposing the person for cancer. Which these doctors did, thus killing at least ten thousand otherwise healthy people. [3]
(By the way, this type of stuff -disproportionate amount of poor people being studied- is still going on.)
“If we studied normal gait now, we’d have to revise everything.”
While she didn’t go into it much, this is the genesis of what Shirley was saying. People move so horrendously now due to the nature of what society has become, if we studied what normal movement is now we’d be completely off.
A low shoulder is something I’ve covered. I’ve seen others talk about this and state, “Don’t worry about a low shoulder. You’ll see something like this all the time. It’s normal.”
When these guys are saying “normal,” I think it’s safe to say we all take that as it’s nothing to worry about. It’s typical for the body to be this way. Like it’s a natural form of being human. Akin to having 10 toes.
To which I say, no, it isn’t. Just because you see it all the time doesn’t mean it’s “normal.” It’s like saying being overweight or sitting 15 hours a day is “normal.” It may be a regular occurrence, but in terms of the health of the body, it’s not normal, it is something to focus on, it is an aberrant condition of an unadulterated body, it is an issue. How the body moves is a reflection of what you regularly do with it. If you have a low shoulder, that’s a reflection of what you regularly do with the arm. (You keep it low.) [4]
We have to be very careful what we consider normal and ok. I’m going to go over this more with the hip later on, but suffice to say, this is not easy. I have no doubt the SIDS doctors were brilliant people with the best intentions…who still killed seven thousand more people than the September 11th attacks…which should scare the excrement out of you.
For a long time we would excise people’s ENTIRE meniscus when they had knee pain. “That tear is not normal.” The result? We destroyed people’s knees by taking whatever good meniscus they had out. Now we try to repair the tear, and if we can’t, we’ll cut a part of the meniscus off. This has by no means been shown as the best approach. We’re finding, in many cases, it may be best to leave the knee alone. (Surgically; not exercise wise.)
Why? Because it’s plausible having some tears here and there is part of being alive for a long time. Not to mention the relationship between chronic pain and structural damage is dubious.
Shirley referenced a guy who had a knee issue for years. Eventually, doctors looked inside his knee, saw how worn out it was, and decided he was a prime candidate for a knee replacement. It was only later, when his knee was still bothering him and Shirley got to work with him, she realized he never had a knee problem; he had a lower back problem. His pain was radiating to his knee, but it wasn’t starting there.
How on earth could a surgeon miss this? Well, remember, when they looked inside his knee; it was really worn out and didn’t look “normal.” But their frame of reference isn’t a 60 year old knee that’s been around the block. Their frame of reference is a perfectly good looking knee. What we need to figure out is, maybe a “worn out” joint is a perfectly good looking knee for a 60 year old. Maybe it’s just like having scars and wrinkles on your skin.
One of the gold standards of research is using a control group as a reference point. How many atypical control groups have we used to deduce what a proper reference frame is? How many imaginary diseases have we concocted? How many futile surgeries are we doing? The scary answer: We have no idea.
Treating chronic problems is a new phenomenon in society. We’ve never had as many people living as many years, and we’re learning on the fly how to deal with this. Alzheimer’s, many forms of cancer, chronic joint issues, these are novel issues for humans. It’s only recently we’ve begun living long enough to have great numbers of people dealing with these things. Up until now we died from infectious disease, malnutrition, violence, all before we had the opportunity to encounter the chronic side of things.
At the same token, it’s not long ago we became such a sedentary society, where physicality is not a major part of our lives.
Let’s take lower back pain as an example. We know 80% of people will have a chronic lower back issue in their lifetime.
How long have we’ve been studying lower back pain? According to Google Scholar, I don’t see a paper referencing something related to “lower back pain” until 1915. And we start to study it more rigorously around the 1920s. We’re less than a century into studying the most common reason people go to the doctor. We’re centuries upon centuries into having a spine though.
Many believe, doctors included, due the prevalence and difficulty in treating lower back issues, it’s a normal part of being human. I’ve seen some state it’s part of the deal for being bipedal. Implying you can’t do anything about it.
How do we know it’s normal? Were 80% of people before the 1900s suffering from lower back pain? What about in the 1500s? Are 80% of people in third world, non-sedentary countries getting lower back pain? Or, is it common (not normal) for a sedentary, long-living population to acquire lower back issues through their lifetime?
In training many different age ranges, I’ve noticed women who are roughly 50 years old and up bend their knees differently than the current generation. You often see women bring their knees together when sitting because of wearing things like dresses and skirts. However, you see this way more often in the older generations.
It didn’t take long for me to repeatedly hear, “That’s just how I was brought up. In my time you never, ever, opened your legs while sitting.” After telling some older women to open their legs when getting up and down to take some stress off their knees, I’ve even heard, “I feel like a prostitute. I don’t think I’ve ever gotten out of a chair like that.”
How easy could it be to study women brought up in this manner, and even nowadays, and conclude squatting with the knees coming in is “normal” for women? Yet, knowing how the Romans and such treated females, I wouldn’t be surprised if there was a time women were ordered to keep their legs spread at all moments. Or, if just before dresses and skirts were invented, women never had to worry about such a thing.
Again, is it normal for women to bend their knees with them caving inwards? Or, is it common for women of the last 100 years to acquire such a pattern?
This is a crucial distinction. Normal, like having 10 toes, well, there’s not much we can, or would want to do about that. Something which is acquired, like lung cancer from smoking, there’s almost always something we can do about that.
In some areas, this type of stuff is obvious. No one says being overweight is normal because two-thirds of population is. In some instances, it’s not that big of a deal either. Exercise someone in the wrong manner and at least they’re still exercising. But, in other areas, it’s extremely difficult to figure out a proper reference frame, and the costs for getting the wrong starting point can be exorbitant.
–
Back to Top
Oddities in knee alignment
Shirley made some remarks on how past meniscal issues can affect current knee alignment.
When it comes to the meniscus, medial issues are more common than lateral issues.

Medial meniscus on left; lateral meniscus on right. (Right knee, top view.)

Right knee, anterior view. (Adapted from http://www.sportsorthopaedicspecialist.co.uk)
When you’re dealing with an older demographic, if they have had a meniscus issue, they probably had a tear which was left alone, or a partial menisectomy. Within that, it was probably on the medial side. Mensical repairs are a newer procedure, and most older people had their meniscal surgery done decades ago. Thus, it was probably a partial menisectomy. (This is worth knowing because most clients won’t remember or know what specifically was done to their knee.)
What you may see with a person like this, especially as they age, is their knee alignment changes to reflect their meniscal changes. Because the medial side has lessened or is gone, the femoral condyles don’t sit on the meniscus like they used to. The person may shift to a varus alignment.
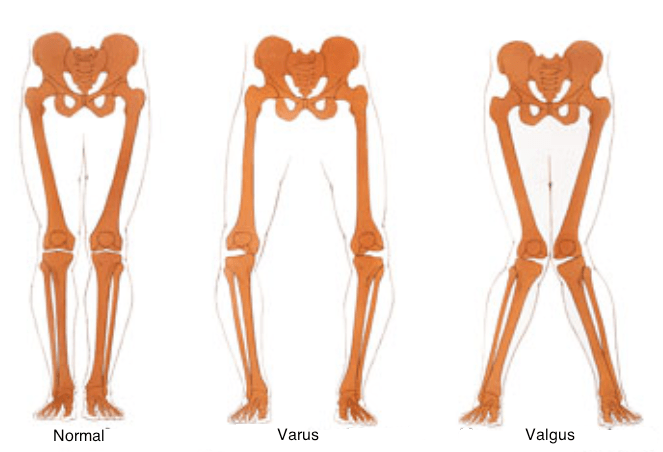
To illustrate this, I’m going to show an example of someone who had their entire medial meniscus taken out. This is often not the case, but it helps for clarity. Because this is tough to visualize, at least it is for me, try using a cup with a ledge to help. One side of the ledge is the intact meniscus, the other is the excised:

You can see how things will change:
Lateral meniscus left in tact; medial meniscus has been removed.
Close up of normal alignment (right leg, anterior view):

Close up of varus alignment:

Note the similarities:


This can go the other way too: Lateral meniscus excision => Valgus alignment. In fact, I have a client with this deformity. Can you recognize which knee had the lateral meniscus partially excised?

The right:

Using the cup again:


There’s that sharper angle at the knee joint now:
![]()
![]()
This is important because you gain an increased understanding of why someone looks and moves the way they do. While I focus with Sharon (pictured above) on not letting her knee cave in, we both understand not to expect it to look like her other knee. We also understand her knee having this now structural issue, predisposes her to not handle certain activities well. Like the racquetball she loves to play. Having a knee with an increased valgus alignment makes her more susceptible for it to collapse inward during activity, which is often how knee injuries happen.
This is the conundrum with many meniscal procedures. While they may give you pain relief in the short term, helping you get back to the activity which likely caused your injury -racquetball for instance- the meniscal procedure could very well make it more likely you injure your knee again, like while playing racquetball.
–
Back to Top
A short muscle doesn’t equal a strong muscle
A mindset I’ve been trying like hell to get people out of is the, “Long =weak; short = strong” muscle view. Where people go, “Ok, this is tight, it must be too strong; I need to stretch it and not strengthen it. Ok, this is weak, it must be too long; I need to strengthen and shorten it.” In a lot of instances, this is true. Not every instance though.
For this post, I’ll ignore the fact this mindset doesn’t include how everything works together (how everything moves), which is what actually matters. Strengthening a bunch of individual muscles and stretching a bunch of other individual muscles gets you as far as Leo at the Oscar’s. You get to be in the conversation, but then you’re D.O.A.
A prominent example illustrating the flaw in something like “This is tight; it’s too strong,” is the gluteus maximus. Atrophied (weak) glutes are readily apparent while standing.
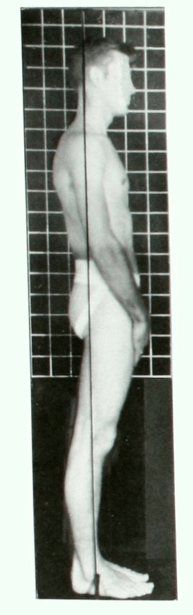
Picture from Kendall’s “Muscles: Testing and Function, with Posture and Pain.”
What’s also readily apparent, is many with atrophied glutes are standing in hip extension.

The glutes are hip extensors. If the hip is in extension, the gluteus maximus is shortened, not lengthened. Yet, they’re atrophied. The muscle is shortened and weak at the same time? Yes.
Muscles contract using filaments, which latch onto one another.
-

Shorten, shorten, shorten, lengthen. (GIF made from this cool video: http://www.youtube.com/watch?v=0kFmbrRJq4w )

If these filaments are significantly shortened, they can’t as effectively contract. There’s nothing left for them to latch onto. They’re at this point in the above clip:

No more room to contract.
If they’re chronically, excessively shortened, the muscle can’t do much, if any, work. It can’t produce much, if any, tension (length-tension relationship), leading to atrophy.

We’re focusing on the left side of the graph right now.
It’s like when someone gets casted up. The muscles in the cast have a hard time producing any tension. Hence the atrophy once the cast is removed.
Furthermore, if a particular muscle can’t do the work it’s supposed to, other muscles pick up the slack. This is why it’s so common for someone whose glutes are atrophied to have lower back issues. Their lower back is trying to pick up the slack. You see the same thing with hamstring issues. If the glutes aren’t extending the hip like they’re supposed to, other muscles which can have this influence will try to help. Like the lower back and hamstrings.
Some might be thinking, “But aren’t the hamstrings, who extend the hips too, also excessively shortened in this case?” Not usually. Because when the hip is in excessive extension, the knee often is too.

And the hamstrings extend and flex the knee. While they have been shortened into hip extension, they’ve been lengthened into knee extension. The rubber band has been tautened from one end but slackened from the other. The filaments aren’t on top of one another like they are at the glutes. In fact, with atrophied glutes often come hypertrophied hamstrings (and spinal erectors).
In someone like above, it’s common to see the atrophied glutes, see the lack of gluteal contraction during an assessment, and prescribe a bunch of glute exercises. Exercises usually involving a great deal of hip extension. 1) You better make sure the glutes are indeed helping the hip extension. Just because the hip goes into extension doesn’t mean the glutes are working. 2) How much hip extension does this person need? They already have plenty of it. You better make sure you’re not going into excessive extension, along with doing other things to work them back into some hip flexion. Their hips need to be flexed a bit before their glutes can effectively produce tension!
This is why it’s typical those with an anterior pelvic tilt have good gluteal definition.


The extra hip flexion can help the glutes produce more tension. Notice the caption in this graph from ExRx.net:
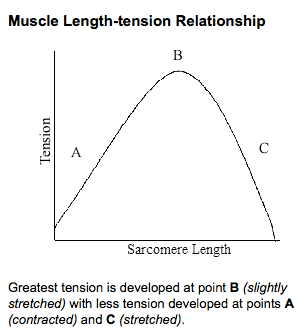
When the muscle is “slightly stretched” is when it can produce the greatest force. An anterior pelvic tilt can slightly stretch the glutes, leading to greater tension ability, leading to hypertrophy. While significantly shortened glutes often become atrophied; slightly lengthened glutes often become hypertrophied. Shortened, or tightened, muscles aren’t always strong, and lengthened muscles aren’t always weak. Sometimes, the opposite is true.
–
Back to Top
Some amazing new surgery, or a sign of the times?
In discussing structural factors affecting movement, we really honed in on the hip. During our lab portion Shirley recognized one girl -who had a back pain history- walking a bit funky. She told the girl to point her toes in a bit, and see how that felt. The girl walks around the room, “That feels better.”
Shirley, “Of course it does. You have anteverted hips. Who told you to walk with your feet straight?”
Girl, “My last therapist.”
Shirley puts her up on a table prone, lets her legs fall out, and sure enough they went out significantly.

Example of femoral anteversion on right side. (Screenshot from one of Bill Hartman’s videos.)
This girl had been, for god knows how long, forcing her hips into a range of motion she doesn’t structurally have. She’s not going to loosen anything up by keeping her feet straight, she’s only going to jam her hip bones together. Does she look pigeon toed / a little weird with her toes in? Yep. Will that help save her from a hip replacement? Yup.
(I’ll get to how a therapist of all people gave her this suggestion, and a therapist, of all people, continually followed this suggestion. To me, (I believe) the only non-therapist in the crowd, this was…disturbing.)
In the last decade discoveries of structural abnormalities of the hip have sky rocketed. To the point I don’t think we can even say what normal is anymore. What we can deduce from these findings is some people are better suited for certain activities than others.
If you have anteverted hips, it’s going to be extremely hard for you to play most sports without significantly risking blowing out your knee(s), destroying your hips, or wrenching your spine. If you have a shallow hip socket, it’s going to be harder for you to do anything too dynamic as you’re at greater risk of dislocating your hip joint. If you have a large femoral head, it’s going to be hard for you to ever safely squat butt to heels, like an olympic lifter, as you’re going to have to significantly round your lower back to get that low. You can’t get the flexion from your hips -the femoral head is too large, so it hits the acetabulum; you end up having to get the flexion from your spine.
It can suck if you end up with something like the above and yearn to be an NFL athlete, but that’s the way it is. Your body is first concerned with survival, then reproduction; not to be optimally put together to dunk a basketball, throw a baseball, or cut on a dime.
People always reference how athletically gifted professional athletes are. While true, we should also acknowledge how structurally suited they are for their sports. You can’t be an olympic weightlifter if you don’t have hips allowing you to fully squat. Furthermore, many athletes who are genetically advantaged for one sport are genetically disadvantaged for another, sometimes due to basic structural differences. If you’re a swimmer, it pays to have a long torso and short legs, like Michael Phelps. If you’re a sprinter, it pays to have a short torso and long legs, like Usain Bolt. Michael Phelps isn’t much of an athlete once you put him on a track; Usain Bolt isn’t much of an athlete once you put him in a pool. (How much of these variations are acquired through adolescence versus given at birth, I don’t know. Nobody knows. I don’t think anyone even has the slightest clue.)
In the grand scheme of life, these are minor issues. Most aren’t concerned with this level of physical performance or these types of ranges of motion past the age of 18 anyways. It’s no different than 99% of us who realize they aren’t tall enough to make the NBA. Stop the activity, modify the activity, or pick something different and move on.
At least that seemed rationale to me.
Shirley started talking about a 15 year old boy who was having difficulty abducting his hips. He discovered this because he had trouble playing basketball. Think a defensive position and shuffling side to side.

The boy also had trouble flexing his hips past 90 degrees.
So, he goes to the doctor with “mild hip pain and stiffness.” When X-Rays were done they discovered the head of his femurs were larger than “normal.” The doctors surmised these large femoral heads were clunking against his acetabulum, giving him pain. They think they can correct this with surgery.
For this procedure, a “femoral-acetabular osteoplasty,” they:
- Cut a ton of tissue to get to the hip joint. It’s not like a knee surgery where there’s not much covering it.
- I don’t know a ton about this, but I believe if it’s open surgery they don’t dislocate the hip, but you have to deal with all the issues open surgery come with.
- If it’s not open surgery, then the hip is surgically dislocated.
- Shave down the femoral neck.
- Shave down the femoral head.
- Shave down parts of the acetabulum. (This boy had some small fractures.)
- Reorient the above structures.
That was the first hip. Post-op the 15 year old was on crutches for ~6 weeks, then he went in and got all the above done again on the other side, after which he was in a wheel chair for a while. 8 months later he was playing basketball again. Shirley closed this story out with, “This is truly some of the marvels of modern surgery.”
I heard all the above, saw the pictures, and was fucking horrified. I don’t consider this a marvel of surgery, a consider this a profound example of a cultural issue. The only reason I can fathom putting your son through a surgery like this is they love basketball / sports, they (or the parents) believe the kid can make it to the NBA, and or they’re worried about their son’s hips as he gets older.
Regarding the last option, if this kid doesn’t flex his hips past 90 degrees and limits how much and often he abducts them, he should be fine. How many people flex their hips past 90 degrees on a regular basis? Most adults I know -other than sitting- don’t flex their hips ever. Why can’t this kid merely make sure to sit in a chair where his hips are below 90 degrees? Same thing with abducting them: Just avoid significant abduction. Is this really crucial for his life between the ages of 18 and 80? No.
Next, as I went over in “If we studied normal gait now, we’d have to revise everything,” there are loads of questions with this type of operation. Especially when it’s so new:
- How do we know this kid could be at risk for issues down the line? Do we have a sample of 75 year olds who we diagnosed with large femoral heads as 15 year olds, then observed them throughout their lifetimes?
- How many people who modify their activities, such as the range of motion they put their hip through, still have issues?
- What are the success rates of this surgery? Are those rates on a large sample size? How many other teenagers have had this done? How are these people doing 30 years later?
- In hip replacements, a smaller femoral head has actually been been shown to increase the rate of hip dislocation. Is the same true for this surgery? Are you (maybe) decreasing the kid’s hip pain by making the femoral head smaller, yet at the same time increasing the risk he dislocates his hip?
- In fact, if a larger femoral head has implications for decreasing hip dislocations, does the kid have a larger femoral head because his body is trying to make sure he doesn’t dislocate his hip while doing activities, like basketball?
- Say there is a risk of hip replacements later in life, is it better to take that risk than the guarantee of surgery now? Is a major surgery like this better when you’re a grown, mature adult, than it is when you’re 15? Is it easier to become temporarily handicapped as a 40 year old than it is a 15 year old?
- What are the chances he has this surgery and STILL needs a hip replacement down the road?
Does anyone think there is a good, solid answer for any of the questions above? I doubt it. My assumption is this kid is very much a lab experiment due to this surgery’s nascency. What we fully know though is this kid has no chance of competitively playing many sports the way he is now. So, I’m forced to deduce sports are the motivation here. Money and fame? Shit, people will do a lot more than be put in a wheelchair for a while.
I don’t know anything else about this 15 year old, who was probably 16 by the time he played basketball again. I do know, by age 15, if you’re still having issues abducting your hips or playing defense, you’re not making the NBA. If the story on you is anything other than, “He destroys anyone he plays against, ESPN is looking at him, he has a ton of college offers already…” you’re not making the NBA.
I know the probability of a high school basketball player making the NBA is 3 out of 10,000. 3 / 10,000 = 0.0003%.When you’re 15-16, can’t play defense, have had two, MAJOR reconstructive surgeries, and missed an entire year of playing basketball, I’d wager that 0.0003% gets a lot smaller.
A recent study looking at elective surgeries examined four million operations over the course of three years. Of four million, about 28,000 didn’t go as planned. 28,000 / 4,000,000 = 0.007%.
3 / 10,000 = 0.0003% chance of making the NBA.
28,000 / 4,000,000 = 0.007% chance of this surgery not going well. (Considering how much more invasive this elective surgery is compared to others, along with how new it is, this number should probably be demonstrably higher.)
0.007 / 0.0003 = 23.
That is, there is a 23 times greater chance this surgery doesn’t go well than there is this kid making it to the NBA. Not to mention he has to do the surgery twice!
Part of this kid’s issue was a large femoral head and neck. This boy is only 15 and still growing. Who’s to say his femur isn’t going to grow right back? Shirley mentioned the genesis for a large femoral head can be playing sports growing up. The extra pounding causes the femoral heads to hypertrophy. Maybe the reason this kid has large femoral heads is because of the basketball he’s playing. Maybe he’s getting a surgery which will help him go back to an activity that caused his issue to begin with.
Actually, since he’s still growing, how do we know the rest of his hip isn’t going to grow to accommodate his femoral heads? When I was little I remember having a big gap in my front teeth. I was easily a candidate for braces. My dentist thought about things and concluded there was a good chance, once the rest of my teeth grew in, they’d push the front teeth together, thus closing the gap. So, after a while, my body would effectively do the job of braces. If not, then we could entertain braces. My teeth came in, pushed my gap together, and that was that. I have no doubt there are an inordinate amount of dentists who would have done the braces to begin with. Our bodies don’t grow in perfect proportion. Some things come in faster than others. Perhaps this 15 year old’s femoral heads have come in quicker than his acetabulum?
And why does nobody think of the psychological impact of doing this to a teenager? I was on crutches for two weeks in high school and I remember them vividly. You feel awful, lonely, and left out. Going around school on crutches is like wearing a Scarlet Letter. People constantly ask you what happened, want to play with your crutches, and generally act like the assholes that teenagers are. Lord knows how this goes over for a teen in a wheel chair. Because of this, you’re likely to rush your rehab. You simply don’t have the patience an older person has.
Oh, I should probably mention what I mean by chance the surgery “doesn’t go well.” By “doesn’t go well” I mean there is a 23 times greater chance he dies in surgery than makes the NBA. Not risk of infection, or surgical failure, or complications, strictly mortality. (Obviously, the chance of general error is greater than any one error alone.)
Sure, 0.007% chance of dying sounds small. 28,000 people dying doesn’t.
–
Back to Top
My conversations with Shirley
A highlight of my trip was the direct conversations I got to have with Shirley.
As far as I know, I was the only non-therapist at this course. Oddly, not many questions were asked. I’m not sure if it was because people were lost (you could tell this course was brand new information for many of the students), it was a weekend course, people were forced to go to this for CEUs, or what, but after the first hour of lecture I thought, “Well, screw this. I didn’t come all this way to not speak” and I started raising my hand. [5]
We were at the beginning of assessing the lower back, talking about standing alignment, and my question was:
“You touched on this in the last slide, and you have a sentence in your book stating to be careful extrapolating certain alignments with certain lower back issues, or really, any lower back issue. That standing a certain way rarely correlates with someone having lower back pain, or the types of movements they do. Could you elaborate on this?”
For those who don’t know, there’s a good amount of research showing standing in a certain alignment doesn’t necessarily cause lower back issues. A particular pelvic tilt is not the devil people make it out to be. This is important because it should be a wake up call to those who obsess over posture. Who pick apart every single thing on somebody, making them feel less coordinated than Lorde’s Grammy performance.

Paranormal Activity 7: The Lordes.
(GIF from CBS / buzzfeed.)
Of course, you have the groups who take this too far the other way. “Posture doesn’t matter at all! Stand however the hell you want!” This is pretty silly. If you make someone with good posture stand with excessively poor posture, you see right away how it can make someone feel. (Like shit.)
Next, what you also find is say someone stands in a posterior pelvic tilt, with their lower back a bit flexed:

What Shirley and I discussed is the above posture doesn’t mean the person has or will have a lower back flexion issue. In fact, even if this person flexes their lower back during many activities, that still doesn’t guarantee flexion is a problem for them. They could very well have an extension issue.
Going with the principles I went over earlier -the site of what moves too much and what direction it moves too much are the pain provocateurs- standing with your lower back in flexion does not mean you 1) Flex your back too much 2) Will have pain flexing your lower back. Standing with your lower back in flexion often means you have pain into extension!
As we age our spinal discs tend to atrophy. With less of a disc there’s less room for our facet joints to move, particularly into extension.


The facet joints become more likely to jam into one another when going through extension.
If you’re someone who has done a lot of lower back extension throughout your life, you can accelerate this process. Just like the tires on your car wear down the more you drive, you may wear your discs down the more you do stupid crap, like obsessing over deadlifting.
It’s natural for our lower back to have a little lordotic curve. This is our spine’s “neutral” to start out with. However, if you’ve become sensitive going into extension, say due to age, or by doing a ton of extension work (oh hey, deadlifting again) what’s a natural response? To keep your back a little flexed. You’re better able to avoid extension, and this way when you do go into extension, you have a little more room before causing pain. You’ve effectively altered your “neutral.”
“But what about a herniated disc? Too much flexion can cause a disc herniation.”
As I mentioned, this isn’t only caused by your movement patterns, age plays a role. I asked Shirley what age she felt extension is pretty much universally contraindicated, “About 60.” Meaning you could have lucked out and had a great back for 60 years, but it’s going to wear out where certain movements still aren’t going to agree with it. (Extension and rotation. Flexion is less of a concern.) This is why you can worry less about flexion at a certain point. Especially in an older person, they don’t have enough of a disc left to herniate! Something like stenosis -extension issue- is going to be much more of a concern.
Maybe now the internet can stop telling me how grandmothers need to arch their back and deadlift more.
–
During a break I went up to talk to her again, this time one on one. During our conversation I was asking her about what’s going on in the pain science world. Bringing up the research of people like Lorimer Moseley’s group. It was cool as we ended up talking for about 10 minutes with a few people watching and listening. Eventually I felt bad as it was our lunch break, so I let her go.
Rather than write a long thing about this part of our conversation, here are the bullet points:
- She has no doubt some people have atypical pain. Pain where there’s no real pattern to it. She hasn’t seen this much herself though. “Now, whether the doctors who referred me patients over the years helped me by only giving me people they figured had a pattern, or those who were already tested for other diseases, I don’t know. Maybe they did.” I got the impression this was more of a, “I’ll admit it’s a possibility, but I highly doubt that’s the case.” Personally, I’m with her on this. It’s so rare I get someone I can’t put into a pattern. And these people have been rheumatoid arthritis patients, fibromyalgia patients, or severe vitamin D deficient patients.
- Due to the difficulty in getting this movement approach to catch on [6], she’s worried the focus on the brain and drugs aspect will lead to over-medicalization. She referenced a young girl she had who was diagnosed with fibromyalgia because she had pain at various points in her body. Shirley was able to give this girl some exercises and corrections and her “fibromyalgia” disappeared. She never had a disease to begin with.
- The research many are referencing is on Chronic Regional Pain Syndrome (CRPS) patients. Shirley believes this is a whole different phenomenon than something like your knee hurting. We talked about how you can still take things away from this research, like just because you have arthritis doesn’t mean you need to be in pain, but you need to be careful about mixing populations.
Shirley did this interview not too long ago, and echoed some of the same sentiments in our discussion:
–
Overall, I’ve been surprised how much trouble the “pain science” world and “movement science” world have had communicating with one another. And some of the hostility that’s ensued. (The hostility is, of course, from the internet, not Sahrmann or Moseley.) Because I’m an outsider to these worlds in the sense I’m not conducting the research and have no skin in the game, I think it’s been easier for me to be objective about this. Where I’m better able to use both disciplines opposed to taking sides. Eventually I’ll write something about this.
Suffice to say, when it comes to everyday people with typical pain: From a practical, how do I handle, what do I do with this person, standpoint: Clear edge movement world. From a deep scientific explanation of what causes a pain response: Edge pain science world. Use the pain science world to explain pain; use the movement science world to treat it (these are complementary!), and we’re looking good.
Shirley and I also discussed the future of physical therapy, which we got on because she was intrigued why I wasn’t a physical therapist, or at the least in PT school. We talked about how the business model may change, the cost of PT school (often too much), impact of Obamacare, etc. It was a cool, sometimes more theoretical discussion.
The next day she made a point to ask me how I was doing when she saw me in the hallway. We talked about shoulder abduction in the obese (I cover that here). She was very generous with her time. All the faculty was. Not only with me but anyone who wanted to ask questions.
–
Back to Top
Getting shorter with age: It’s not just the spine (why your pants are longer now)
Shirley had a funny anecdote about how for a long time her patients would tell her, “I feel like I’m getting shorter.” No problem, she knew why that was occurring (the spine). Sometimes they’d also go, “My pants don’t fit me now. They’re too long.” She chalked that up to them being a little senile. Pants getting too long? That doesn’t make sense.
Turns out, it does make sense.
At the top of the hip, the bones will endorse one of three angles. Normal, coxa vara, or coxa valga. You know I like my fancy terms; let’s reword this as, “Normal, angled lower than normal, or angled higher than normal.”

Shirley stated it’s been found our hips take more of a coxa vara, “lower than normal angle,” as we age. After you’ve been around 6-8 decades, gravity tends to win.
Say we start out like so:
 That starting incline can decrease with time, bringing the waistline along with it:
That starting incline can decrease with time, bringing the waistline along with it:

Looking at the bottom, you can see how the pants lay over more and more of the foot. While the length between the person’s feet and waistline has changed, the length of the pants hasn’t. Denim doesn’t shorten with time. Alas, “My pants are too long.”
–
–
[1] I discuss how getting rid of arthritis in the knee doesn’t alleviate pain in this post: Should you have surgery for arthritis in your knees?
[2] An example of one outlier, where many chalk it up to “a shitty hand”: There is a great book called Survival of the Sickest by Sharon Moalem. Per the title, the book looks at why people who get sick are still in the gene pool. Shouldn’t they have been weeded out by now? There’s no good in having a disease. Why on earth would someone get something like Type 1 diabetes?
First, if a disease doesn’t preclude you from reaching a point in which you can reproduce, it can be passed on. We could all have a disease that kills us by 30, but if we reproduce before 30 years old, our kids can inherit the disease.
Second, and this is where the book gets trippy, maybe these diseases are why some of us are here to begin with? Maybe, without Type 1 diabetes being in your gene pool, you would have never made it here? Type 1 diabetes is…beneficial?
One of the symptoms of Type 1 diabetics is a lack of insulin production, leading to excessive sugar in the blood. Another symptom is frequent urination. As a Type 1 diabetic you’re likely to 1) Have less water in your body than someone else and 2) Have more sugar in your body than someone else.
Moalem covers how we’ve found a good deal of Type 1 diabetics appear to have heritage tied to surviving extremely cold weather. If you’re a Type 1 diabetic in an ice age, you possibly have less water in your body due to your more than normal urination. Less water in your body = less substance in your body which can freeze and kill you.
Next, the excess sugar in your body can help act as an antifreeze. Moalem references how grapes which survive colder weather do the same thing i.e. have increased amounts of sugar. This is well documented because these grapes end up sweeter. (They’re popular in the wine community.) The plethora of sugar in a slurpee is a good example too. Think about the ice in a slurpee versus a cup of water. Shriveled, soft ice compared to solid, hard ice. Soft ice is a lot less damaging than hard ice. Plus, it warms faster. Say you’re a grape with some ice crystals inside you from cold weather. If you have more sugar inside you, that ice can be made softer, thus warm faster. The faster you can warm yourself up, the better.
So, while Type 1 diabetes may, in certain circumstances, make it so you don’t live as long as a normal person, it at least gets you to an age you can reproduce. An age you may not have gotten to without the disease (you would have died in the ice age). Thus, Type 1 diabetics are still around.
The book has more examples. Lord knows how many ailments fit in this category.
[3] Perhaps the greatest irony of the SIDS story is the well off were the ones who had a lot to do with poor people’s bodies being donated to medicine. They went so far as to have laws if you couldn’t afford a proper burial, the body was automatically donated to medicine. Who was most likely to experience these irradiation therapies? Those who could afford it, i.e. the well off.
Maybe karma does come back around.
[4] It’s typical in the research world to hear how outdated some research might be. While older research may be crude, the fact it’s older and may have studied a different population could prove fruitful. If Florence Kendall were to conduct her work now, who knows how different -and potentially wrong- it would be. She could have thought a low shoulder was normal herself.
[5] A good example of why sometimes paying for information is better than free. I was shocked how many students got to go to this course for free, because their employer paid for it. At the same time, I was shocked how uninvolved many students were. I paid a nice chunk of change to go to this, I wasn’t going to waste it.
[6] Along with the interview I linked above, Shirley discusses the difficulty in getting her method across in this video:
–
We touched on some different aspects than this video, but here’s her talking about the future of physical therapy:
–








Posted on June 16, 2014