
I’m going to reference Scapular winging: anatomical review, diagnosis, and treatments often.
–
Anatomy of scapular winging (muscular)
Serratus anterior
Of course, we have to start with this muscle.

The serratus anterior protracts and upwardly rotates the scapula.

Let’s use a nice quote from the paper to get more specific. Pictures and bolding from me:
“The serratus anterior is a broad flattened sheet of muscle originating from the first nine ribs and passes posteriorly around the thoracic wall before inserting into the costal surface of the medial border of the scapula.
(Fancy talk for it goes from the ribs to the scapula.)
The serratus anterior has three functional components. The superior component originates from the first and second ribs and inserts into the superior medial angle of the scapula. This component serves as the anchor that allows the scapula to rotate when the arm is lifted overhead.
The middle component of the serratus anterior originates from the third, fourth, and fifth ribs and inserts on the vertebral border of the scapula, serving to protract the scapula.
The inferior component originates from the sixth to ninth ribs and inserts on the inferior angle of the scapula. This third portion serves to protract the scapula and rotate the inferior angle upward and laterally.
As a whole, the main function of the serratus anterior is to protract and rotate the scapula, keeping it closely opposed to the thoracic wall and optimizing the position of the glenoid for maximum efficiency for upper extremity motion.”


It’s not just about the serratus anterior
The serratus anterior is not the only muscle impacting a winging scapula. When a scapula wings it’s because it isn’t held close to the rib cage. The serratus anterior gets a lot of attention because it’s anterior to the scapula, and attaches to the scapula. When a scapula wings it often displaces posteriorly. Naturally, the thinking goes the serratus anterior is “long and weak” because the scapula isn’ t being held close to the ribcage.
However, other muscles connect anterior to the scapula, and connect to the scapula.
Trapezius

Because the spine is ventral to (in front of) the scapula the trapezius can pull the scapula a bit anteriorly. That is, closer to the ribcage.
Parts of the trapezius also fall on top of the shoulder blade.

If the trapezius is on slack, or not firing properly, the compression on the scapula lessens. Making it more likely the shoulder blade won’t be as tight to the ribcage, aka wing.
Rhomboids
For many of the same reasons above, the rhomboids can play a role in the shoulder blade winging too. Because this is so rare (the authors go over this too), I’m not going to cover it.
Position of the scapula
Due to the attachment sites of the above muscles, we can get a good feel for which muscles need work by the position of the scapula. A nice chart from the paper:


Right scapula front view.

Right scapula back view.
Right shoulder winging due to issues with the serratus anterior (it gets progressively worse):

–
See how the scapula is traveling excessively medially and superiorly?


Winging due to issues with the trapezius:

From the paper: “Notice the lateral displacement of the scapula with the superior angle more lateral to the midline than the inferior angle.”
An important note here: I don’t think it’s feasible to fully separate these two impairments. When a serratus anterior issue is present it’s pretty much guaranteed there’s an issues with something like the trapezius. For instance, while this has serratus issues:
You can see issues with the trapezius as well. The superior angle (where the trapezius attaches) is lateral to the inferior angle. A sign the trapezius is also not firing like it should be.

–
Anatomy of scapular winging (nerve)
Long thoracic nerve
Much like the serratus anterior, of course we have to go over this nerve. The long thoracic nerve is part of the brachial plexus.

The brachial plexus is a group of nerves which run down from the neck, under the clavicle, connecting to various points around the shoulder. 
-Image credit and copyright to Kenhub (great anatomy site!)
The long thoracic nerve connects into the serratus anterior:


Because this nerve is what gets the serratus anterior to fire, and people with scapular winging often have so much trouble getting their serratus to work, the long thoracic nerve gets a lot of attention. However, attacking the nerve doesn’t get us anywhere. We need to go after why the nerve has a problem. Why is it having trouble firing, thus the serratus anterior is having trouble firing. The nerve doesn’t just sporadically stop working one day.
–
Figuring out the cause of scapular winging
“The serratus anterior is weak” is not a cause. “The long thoracic nerve isn’t working” is not a cause. Why are there issues with the serratus anterior? Why did it become weak? Why is it not firing properly? Why is the long thoracic nerve not helping?
Muscular
As I went over above, we’re primarily interested in getting the trapezius and or serratus anterior to work better. Muscles which help hold the scapula to the rib cage and lift (rotate) it upwards. With that, it’s logical to assume muscles which perform the opposite functions -pull the scapula away from the rib cage and or rotate it downwards- are likely working too much. Muscles such as, but not limited to, the rhomboids or pec minor. We want to calm them down. If they’re too active they can limit the ability of the trapezius and serratus anterior to do their jobs.
Nervous
We’re interested in anything which could limit the ability of the long thoracic nerve to fire. We’re primarily concerned with compression of the nerve. From the paper (when discussing the long thoracic nerve):
“Proposed vulnerable sites for injury include compression of the nerve between the clavicle and first rib and traction within the nerve’s fascial sheath.”
The clavicle and first rib may come closer together pinching the long thoracic nerve between them.

In my experience, this most often manifests with the clavicle / shoulder drooping.

Which goes hand in hand with our discussion of muscles pulling the shoulder down. The overactive muscles which may cause a shoulder to droop, are the same muscles which oppose the serratus anterior and trapezius.
This is the long way of saying you can’t really separate nerve issues from muscular issues. They work together. Granted, I once saw a woman who had her long thoracic nerve severed because of a mastectomy. Her winging was truly a nerve problem. But that’s the rare case. We’re more concerned with our average person.
So, how do these certain muscles become dominant? How does this nerve get compressed?
–
Daily activities causing issues with scapular winging
I’m going rattle off a bunch of scenarios where the shoulders are being depressed / downwardly rotated.
Bra Straps
The downward pull of bra straps can cause the shoulders to become depressed over time.

This is especially poignant for those who carry a considerable amount of weight in their bra.
Carrying heavy objects

Much like the bra strap comments.
Computer Posture
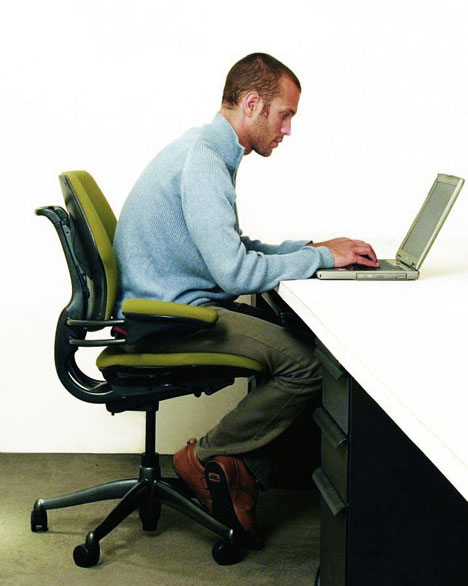
The forward head posture causes the levator scapulae (downward rotator) to pull on the scapula
The internal rotation (hands / arms turned down and in) can cause stiffness in the pecs and lats. Both of which can limit our ability to get our arms up.
Leaning on elbows

Notice the right shoulder protruding
This can push the shoulder into retraction, stiffening the rhomboids.

Next, this can indirectly cause winging. When leaning on the elbows the humerus can become displaced anteriorly (forward) and or superiorly (upward), lengthening the subscapularis.

A muscle which depressed the humeral head, pulling it posteriorly (backward) and inferiorly (downward).
When the subscapularis is lengthened it may shut down causing other humeral head depressors, such as teres minor and infraspinatus, to work more than they should.

These muscles can then stiffen up. This stiffness may appear when someone internally rotates their arm. Notice the winging during internal rotation here:

Credit to Diagnosis and Treatment of Movement Impairment Syndromes (Great book!)
I didn’t go over this in the initial anatomy section, but stiff external rotators of the humerus can cause winging as well. Because these external rotators connect 1) anterior to the scapula and 2) to the scapula, similar to the muscles I went over earlier. The difference being these muscles internally rotate the scapula (away from the ribs), while the others externally rotate it (close to the ribs).

–
Standing with hands on hips

This goes hand in hand with the above. The internal rotation causes issues with the lats and pecs, and the elbows behind the humerus promote anterior translation of the humeral head (stretching the subscapularis). All these muscles pull the arm downwards as well. Something we want to avoid in exercise too.

–
Exercise routines causing issues with scapular winging
Too much pulling
Exercises such as DB rowing, chin ups, lat pulldowns, chest supported row, all work on muscles which downwardly rotate and retract the scapula, as well as extend the humerus. Muscles like the rhomboids, lats, teres minor and infraspinatus. As we’ve seen, if anything, in someone with scapular winging we want to atrophy these muscles.
Too much work in horizontal plane
Horizontal meaning the arms move forward (in front of body) and back (behind body), rather than up (overhead) and down (below head).
Going with that, horizontal pushing exercises, such as push-ups, bench pressing, DB bench pressing, all work the pecs to a great degree. Muscles we again want to calm down.
Yes, it’s true some scapular protraction is present. But this is where we go back to the function of the serratus anterior.
“the main function of the serratus anterior is to protract and rotate the scapula”
And there’s minimal, if any, upward rotation in any exercise only taking place in the horizontal plane. Now we can see why something like the push-up plus exercise is pretty much futile.

{kind=link}
{kind=link}

Some people will lift the arms up a bit higher to place the shoulders in more of an upwardly rotated position. If you want to really upwardly rotate the scapula you know what you could do even more of? Lift the arms higher. Like, all the way up. Isn’t this the goal anyways? To be able to lift the arms all the way up?
Furthermore, exercises like the push-up plus and others may promote scapular protraction while simultaneously promoting scapular retraction.



–
Whatever you may be promoting in scapular abduction (protraction) you’re offsetting with adduction (retraction). Something you rarely want in a scapular winging issue, or most shoulder issues for that matter.
Note the similarities:
Pain during arm elevation due to excessive scapular retraction:

Looks pretty similar to the position of a push up plus:


Sure, you could cue around this (I rarely ever see someone do so), but you still have to account for the fact upward rotation is not being sufficiently attained.
Lack of overhead work
What you end up concluding is the way to solve these types of issues is not to avoid overhead work, but to embrace it. Overhead work enables us to:
- Fully utilize the serratus anterior and trapezius (upward rotators and preventers of winging)
- Stretch the pecs, lats, rhomboids, levator scapula (downward rotators)
- Stretch the infraspinatus and teres minor
This doesn’t mean you immediately start forcing your arm overhead. Some people need to very slowly work on their overhead range of motion. I’ve seen many a people who could only go a couple inches before their pain kicked in, and that’s ok. We don’t push into that pain, and we’ll see the range of motion improve with time.
Forcing me to disagree with this statement from the authors:
“Upon diagnosis, patients should be advised to avoid overhead use of the effected extremity and to avoid activities that cause pain.”
It’s not so much what you do, but how you do it. It’s not so much you shouldn’t bring your arms overhead, it’s how you go about doing it.
You’ll never be able to get your arms vertical by only working them in the horizontal.
–
If you’re looking for some other steps you can take to help with scapular winging, specifically during the day, such as while typing and sitting, you may be interested in this.