We have muscles which pull the knee cap (patella). Some of these muscles pull the patella upwards, like the quadriceps.

Sometimes it’s hard to appreciate how all these muscles connect with the patella from drawings. Let’s look at a cadaver:

P = Patella; ITB = Iliotibial Band; RF = Rectus Femoris; VL = Vastus Lateralis; VM = Vastus Medialis ( Credit: http://jbjs.org/content/88/9/2042 )
(If anyone thought for a second, “Wait, do I have metal in my body?” you hopefully don’t!!)

C, D, and E are quad muscles. Credit: https://o.quizlet.com/0mgvtpi9zV035JqwC53E4w_m.jpg

Some of these muscles pull the patella in (medially), like the inside of the quadriceps, the vastus medialis. Often referred to as the VMO (vastus medialis oblique):

(There is also a rotational impact, which you can hopefully see above.)
And some of these muscles pull the patella out (laterally), like the vastus lateralis:

This has been the most talked about aspect of patellar tracking. “The vastus lateralis is stronger than the vastus medialis, so it pulls the patella sideways.” (Tracking issues virtually always encompass the patella moving laterally, not medially.)
Without getting into the depths of this, long story short, we can’t really selectively recruit the vastus medialis to even out this imbalance, even if it were there. Many, many researchers have assessed many, many exercises. Maximal activity wise, the muscles are often the same. If there is a difference, it’s not worth worrying about. If anything, you can pick a lot of exercises which don’t recruit the vastus lateralis more than the vastus medialis, the ratio being even, but we can’t pick things which activate the vastus medialis more than the vastus lateralis.
However, when the muscles turn on can have an impact. If both turn on the same amount, but the vastus lateralis turns on before the vastus medialis, then we can see how the patella may end up tracking improperly.
Vastus Lateralis on left; Vastus Medialis on right:

Notice the patella moves up and laterally first as the vastus lateralis activates first, then moving further up and somewhat medially, once the vastus medialis kicks in.
In other words, it’s pretty much a waste of time to be focusing on which exercises you’re doing in this regard. Ironically, this is where too many have placed the emphasis. What isn’t a waste of time is working on how you perform exercises.
Some research on this:
–Here
–Here
–Here
There is also some research going over how this has been disputed:
–Here
–Here
The second study above is intriguing, as the VMO was taken away from rabbits, finding not having a vastus medialis didn’t impact various metrics. It’s not exactly applicable, as the way the muscles were then contracted was through stimulating the nerve (rather than volitional contraction), and rabbits aren’t people, but it’s one way to go about looking at it.
Like I said though, we’re not going to get into the weeds on this.
Anyways, this brings up one of the common pitfalls of research nazis: We too often want EVERYONE to fit into the same cause of a problem. A good deal of people with patellofemoral are going to have issues with their VMO timing. But a good amount won’t. So, we do a few things to work on the VMO, but we don’t obsess over it, or only work on that. Your kneecap can hurt for more than one reason.
This is a client I worked with briefly, who before working with me, noticed their quadricep firing patterns were different. Their left knee had been giving them issues, but the right knee had not.

What they noticed and what you can see above, is on the left side the inside and outside of the quadriceps fire at about the same time. On the right side, the inside fires first. Remember, the left side is where this person had pain. Once they straightened this out, their pain went away. So, in this person’s case, the VMO firing before the VL helped out. Nothing strength wise was really needed though. As you can see above, those quads look thick, and damn symmetrical size wise.
Again, no need to obsess over this. We do some things to work on activation, but we also look elsewhere.
–
Another structure which pulls the patella laterally is the iliotibial band:

In blue, with the black outline showing how the band starts high, but connects down into the knee cap.
However, the IT band is not a muscle. It’s a band of tissue, which has multiple muscles connecting into it.

Credit to Anatomy Trains and Tom Myers

These muscles, most notably the tensor fascia latae (TFL), can get stiff, causing the IT band to be stiff, causing the patella to get pulled laterally.
This is the less commonly referred aspect of patellar tracking issues, though one could argue it should be the most talked about. “IT band = stiff; VMO might be lazy.”
If we put someone in a position to stretch their tensor fascia latae and iliotibial band:

One example. You can read more about this here.
In those with knee issues, like pain around the knee cap, they’ll often get pain during this. (Note the word often. Again, plenty of people have knee pain without having IT band stiffness.) One way we can see the IT band is stiff during this (as well as other musculature, like the rectus femoris (a quad muscle)), is the leg will not lay parallel to the floor:

->If it does lay fairly low, then often it’s by compensating through letting the leg fall out to the side. (The TFL pulls the leg out (abduction).)

Where once we bring the leg in (green line above), then the leg will rise up some and or there will be some kneecap pain.
The other way we can see the IT band is at play is if we push the patella medially (during the stretch),
The pain goes away, or at least will significantly reduce. It’s hard to get much more clear than that…the IT band, and TFL, need to be loosened up, and the patella tracking laterally is causing pain.
Example of the mobility of the patella, in a side to side fashion:

But this still doesn’t give us why. It tells us what’s happening, but why does this happen? Furthermore, can there be more to it than this?
–
Genetic factors
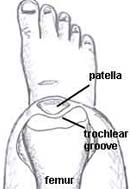
The patella sits in something called the trochlear groove:

Found here: http://orthoinfo.aaos.org/figures/A00707F01.jpg

Knee cap removed (Found here: http://optimumsportsperformance.com/blog/wp-content/uploads/2009/03/1kneetrochleargroove1.jpg )
In patellar instability, or someone suffering chronic knee cap dislocations, the patella is falling out of this groove. This is a more extreme version of our patellar tracking issue we’ve gone over.


Not fun!
Let’s start with a simple one here: The deeper this groove, the less likely the knee cap is to fall out of it. Some people are going to have deeper grooves than others. Those with a less deep groove we say have trochlear dysplasia. You know that thing you hear about in dogs? With their hips? Same idea. Dysplasia meaning the joint isn’t as deep as we’d hope. This can happen in any joint. The deeper the joint, the more stable it is. (In exchange you may lose flexibility.)

Variety of forms of trochlear dysplasia. Sometimes it’s not as shallow, sometimes it’s not shallow at all, sometimes it’s an odd shape.
Next, we hope this groove is fairly symmetrical. In humans, the lateral ridge will usually be higher, but that’s ok, as lateral instability is what we most worry about. If they’re the same height, or if the outside mountain is lower than the inside, we make it easier for the patella to fall outside of the valley.
Normal-

Lateral ridge flattened-

![]()
Making it easier for the patella to fall that way-
![]()
The patella is controlled in large part by the quadriceps, which connect into the patellar tendon. This tendon connects into the tibial tuberosity, just below the knee:

If this tuberosity is say, off to the side some,

Then this is going to change where our patellar tendon inserts:

Which will change our line of pull. When the quadriceps exerts its pull on the knee cap, it can subsequently pull the knee cap out of the groove. Or at least be more likely to.

Notice on the left the line goes straight through the patella, whereas on the right it’s offset:
![]()
On the right picture, the lateral side of the patella will subsequently be compressed more, as that side is being pulled on more. Increasing patellofemoral contact forces in one spot is a good way to piss the knee off. It also makes stability issues -keeping the patella centered- more difficult.
-> This is where we unfortunately realize not everyone has the same anatomy, and not everyone’s anatomy can handle the same forces. If you’re engaging in an activity requiring a lot of force at the knee (deep squatting, running with deeper knee bends (e.g. soccer)), but have this type of anatomy, your knees may start barking at you much earlier in life than otherwise.
All of these structures can be dealt with surgically. I witnessed a veterinarian surgeon perform all the above on a dog (remarkably similar knee anatomy), and it is an intense surgery. We’ve come a long ways surgically when it comes to making things less invasive. The arthroscope being the main innovation. Well, this often entails not using an arthroscope, and cutting half the leg open! (Increasing the risk of infection.)

Taken from this video: https://www.youtube.com/watch?v=dyuiuZvJlTU

No surgery is a surgery you want. But this is one you really don’t want. As in the case of moving the tibial tuberosity, reshaping the trochlear groove also entails a literal saw. I witnessed the surgeon moving his hands back and forth with a saw as if he were lining up a 2×4.
(In the case of moving the tibial tuberosity, if the above picture doesn’t do it for you, enjoy this video.)
–
Femoral anteversion is another factor with all this. As a quick recap, femoral anteversion is when the thigh rotates inward more than usual. (Here for a more in depth discussion.)
If we’re looking at the top of the hips, downward:

Front of the hips is at the top of each photo; back of the hips is at the bottom of each photo.
Because the thigh rotates inward more than usual, the knee comes along.


Keeping our tibial tuberosity structure in mind, if we rotate the thigh / knee in, but keep the tibia at the same place:


We again end up with that lateral line of pull:
Center image has line going through middle of patella, while outside images have line offset.
Instead of moving the tibial tuberosity laterally, we’ve moved the femur internally. But in effect the same thing has happened. The tibia, relative to the femur, has moved laterally. And often it will be more than this. Rather than the tibia staying in neutral, it will often rotate compensatorally. If the femur is in, the tibia / foot tends to move out.

Notice the feet (and tibiae) turned out, with the knees turned in.
In other words, our trochlear groove is even more inside of our tuberosity. Making our line of pull even more lateral.
Femoral anteversion is something which can also be dealt with surgically, but the same earlier caveats apply.
Furthermore, none of these surgeries seem to be common. At all. At least not in humans.
-> An exception to this is the iliotibial band. A procedure which became very common is called a lateral release, where the IT band (and more) is cut in a way to attempt to loosen it up. Think cutting out the middle of a rubber band, so it’s not as strong. This is falling out of favor some as we’ve learned going after why the IT band gets stiff is more beneficial than solely addressing if it’s stiff.
Whether surgery is indicated is a case by case situation. In dogs, this type of stuff, patellar instability, tends to start often in life, illustrating the congenital aspect. (It can start after a traumatic event as well.) Watching a surgeon dislocate the patella on a dog, seeing how easy it happens, understanding a dog doesn’t have the volitionality a human does, surgery makes more and more sense.
But with humans, you run across these types of people, and by the late teens or early 20s, or not too long after a traumatic event, most will know exactly when their knee cap dislocates. “If I move my leg like this, I can pop it out and in easily.” So first course of action…don’t do that movement.
-> If you’re into sports, and you’re having knee cap stability issues, it gets tougher to get away with no surgery. You’re likely going to end up in some vulnerable positions, with a significant amount of force being applied to the knee cap. In sports, you’re reacting to your environment, whereas in everyday life, you’re more able to consciously go through it. This is where a serious consideration needs to be made in regards to the cost / benefit of surgery, vs something like modifying your activity.
And dislocations are a much more rare form of patellar tracking issues. Genetics may play a role, but how we move likely plays a bigger role, for most.
–
Getting back to (functional) causes (things you can do something about!)
Now that we have our anatomy sorted, we can reconstruct the situations which put the leg in a vulnerable position, such as the tibial tuberosity outside the trochlear groove (said simpler: when does the knee turn in and or the shin turn out?) and get rid of those situations.
For example, when laying down, we don’t want the knee to be inside the tibia. We don’t want that trochlear groove (knee) medial to the tibial tuberosity (shin).


This might be more clear for some if we rotate the image:

Same would go for sitting.

The feet turned out here indicates the tibiae are turned out.
This is a really common position men sit in:

Think about it. For too many, sleeping is ~7 hours; sitting is ~14 hours. That’s a lot of hours to place your knee(s) in that position.
-> Plus, as the knee bends to 90 degrees, the stress on the patellofemoral area goes up dramatically. Even sitting like this for hours and hours isn’t the best:

Whenever you get up and down from a chair, or whenever you do a squat in the gym, maybe you’re like this:

Notice the knees caving in. Many women do this when wearing certain clothing, like a dress or a skirt.
When you walk or run, does the foot (and tibial tuberosity) turn out like this?

–
What to do
- We can perform exercises which loosens up things like the tensor fascia latae, IT band, as well as the quads.
- Loosening up the quadriceps can be advantageous because when the quads pull on the knee cap, they compress it. By slackening them some we can lessen how much they are compressing the knee cap.
- If the knee cap is a bit loose (not very stable), then actually some strengthening would be advantageous. (We end up doing some stretching and strengthening together.)
- Attempting to strengthen something like the vastus medialis is tougher. In something like a squat or leg press, when we work that muscle, we also work the vastus lateralis, which opposes the medialis. We would want the vastus medialis to get stronger relative to the vastus lateralis. We don’t want to just make them stronger.
A better way to approach this is to worry about the vastus medialis firing properly. As alluded to earlier, a lot of has been done to see which exercises work the VMO more than the VL. Or some variation of that research. All with little to show for it. But that’s not so much our concern here. Our concern is not how strong the VMO is, but when it contracts. We don’t want it to be lazy, then all of a sudden rushing in at the end, trying to make up for lost time.
Furthermore, while it’s true trying to get the VMO to fire considerably more than the VL is pretty much an exercise in futility, there are positions which work the vastus lateralis more than the vastus medialis. Those would be things we’d want to avoid.
- At the same time, we would want to embrace exercises which help us realign our leg. Exercises which help get us out of the knee(s) turning inside the foot. So we could ingrain a new habit which gives our kneecap a better chance of staying centered.
- Finally, we want to not only focus on these things during exercise, but during the other 23 hours of the day. Modifying how we lay down, sit, and move around.
The above is part of a manual called Mitigating Patellar Tracking Issues.
-> Mitigate is a carefully chosen word here. Remember, you may have some genetic predisposition to have a particular type of structure, whereby completely alleviating a patellar tracking issue, or your susceptibility to it, is impractical. That said, getting to where you can get through your day, and exercise, is almost always feasible. (If it wasn’t feasible, you probably would have had surgery for something like a dislocated kneecap already.)
The manual comes in the form of a password protected link, with various sections-
- Activities of Daily Living
- Notes for laying down (like sleeping), sitting (like at a desk), and moving (like walking)
- Exercises
- Videos of all the exercises, with voiceovers discussing technique
- Cue reminders for what to think about during each exercise
- Rationalization- The reasoning behind the exercises. If you’ve read the above, it should click fairly quickly, but this will reinforce the why behind the exercises. This will also provide a framework for picking your own exercises. Note this is not heavy anatomy, but one to a few sentences illustrating why an exercise is indicated. (If you ever want more know how, email me.)
- All the exercises can be done at home, using common items found in any house (or apartment). No extra equipment is needed. Not even a gym membership.
- Monday – Sunday
- An example of what to do each day of the week. Warming up, exercises, sets, reps.
- Footwear
- Some brief words on shoes to be careful about, and why
The manual is $12, and can be bought here (you’ll be redirected to a Paypal check out but you do not need a Paypal account):


After purchasing you’ll be redirected to the password and link, as well as receive an email confirmation.
If you ever have any issues, email me directly, b-reddy@hotmail.com. I read and respond to all emails. Hope it’s helpful!
–







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Chiru Adrian
March 21, 2016
Hi.
I found that I had “runner’s knee” a few weeks ago.
As I searched the internets the same thing came up. VM too weak etc etc. I though to myself this can’t be right since I can squat 130 kg. Anyway I tried rehab for quads. 2 weeks wasted, pain still there. So I looked at It band as the next culprit.
Found this stretch
https://www.youtube.com/watch?v=x30rjVT-TLo
Decided to do it and what do you know
Pain dissapeared instantly after the stretch. I could bend my leg pain free with literally 10 minutes of stretching. Obviously it came back after a while but 1 week of this and I started running again. Any discomforts were quickly gone after stretching. So in my case the culprit was a tight TFL
This article should be more widespread
reddyb
March 22, 2016
Hey Chiru,
Thanks for the nice words. You actually might be interested in this article. Bit more specific and focused as to the anatomy of the IT band and TFL, and how that impacts stretching it in the context of how many people with TFL stiffness move. The guy in the video is making a common faulty assumption- http://b-reddy.org/2012/03/04/the-best-damn-it-band-stretch-ever/
The stretch in that video could also be hellish on some people’s hips. Not everyone has a hip structure that can get into that position. Something to be careful about. Forcing that position on hips which structurally can’t get there could really tick the hip(s) off. Though sure, for some, it’s going to feel quite nice. The stretch he shows is really stretching certain parts of the glutes.
Chiru Adrian
March 22, 2016
Thx for those. I make sure to never force that stretch as its pretty intense. I just let my legs fall naturally and take my time with it. Usually 10-15 minutes per leg. I make sure to warm up though just in case. Pulled a muscle a few years ago stretching cold. Never again. I agree that some people confuse stretching sensation with impingement of bones so that would be bad and should be avoided. I’ll try the stretch in your article and see how it goes.
reddyb
March 25, 2016
Sounds great. Best of luck.
Tom
December 22, 2016
Hello Brian,
First off, a word of thanks to you for such an informative and well-researched website! I am fairly inclined to follow your advice, but may I ask you a few questions first?
The patella on my left knee is badly shifted outwards (patellar dysplasia), to the point where there’s no cartilage left on the lateral side and my patella pretty much touches the femur. Consequently, I am not able to do any sport that involves intense work of the thighs, cycling included. The pain starts when I bend my knee at, say, 20 degrees and continues all the way to about 90 degrees. I have done some physical therapy (mostly knee-light stuff like straight leg raises, thigh contractions), shockwaves, etc. and, needless to say, to no avail. I’ve also been doing foam rolling daily for months now (I’ve read about your position on foam rolling). Plus, I started doing unweighted squats on my own a week or so ago, and surprisingly I am able to do them, even if obviously it hurts (I got my inspiration from the following site: http://www.kneestrength.com/unweighted-squats-knee-pain/, so my squats look something like on that site, except that I try to do them in slower fashion (hurts a bit less) and I keep my feet as parallel as possible, which the ‘kneestrength’ guy also advises to do somewhere in his guide. My VMOs are very weak, but I feel them working hard during the squat, which makes me think I might be doing the right thing.
So on to my questions at last:
What’s your take on the kind of squats I do? Do you think there is a realistic chance my knees could improve considerably? Would your manual above and the one on IT band stretches address my condition?
I am a 36-year-old male, normal weight. Pretty much the same as above also goes for the patella on my right leg, even if that hasn’t been proven by an MRI examination yet.
Thank you in advance. Please feel also free to shoot me an email if you deem that more appropriate.
Tom
reddyb
December 23, 2016
Hey Tom,
My position on your squats would be if it’s painful, avoid it. One reason squats could be painful for someone like you is because the patella isn’t tracking properly. But doing the motion then means you’re promoting maltracking. Going into the movement, e.g. patella lateral tracking, doesn’t typically help avoid the movement. You’re continuing to groove that dysplasia pattern.
The article you reference mentions going above a depth that’s painful. I’m a fan of this.
Feet positioning won’t dictate VMO activation, unfortunately. I will do some work with people with the feet parallel, but that gets a bit technical. Something I should probably write a post on. In general though, I let people squat with whatever foot position is comfortable for them, so long as they are able to control the knees from turning inwards.
For the manuals, there would be a lot of overlap with the IT band and tracking manual, where just the tracking should be sufficient.
In terms of knowing what can happen with you, that’s really hard to answer. An assessment would first be needed (https://b-reddy.org/2013/06/20/the-remote-client-process/) and even then a lot of factors go into that. Discuss this some here- https://b-reddy.org/2013/08/01/how-long-does-it-take-to-get-rid-of-chronic-pain/
My initial concern would be how far along is your dysplasia. Regardless, a non-surgical approach is what nearly everybody wants to start with -what you described as exercise / therapy so far isn’t enough (not saying that’s your fault)- but there are people who are “so far gone” that surgery is indicated. Can be very hard to know where that line is.
That said, I haven’t worked with anybody who couldn’t get to a pain free squat.
Joseph Phillip Danna
November 5, 2017
Hey Brian thanks for such an intensely descriptive lesson. Keeping in mind that all the imbalances and circumstances mentioned must play a part, for someone with bone-to-bone knee arthritis, would the general thing to stave off a knee replacement be to accomplish decompression of the knee joint, even if only for temporary relief? Not looking for dx, but generally speaking. This woman is bowlegged. Thank you.
b-reddy
November 5, 2017
Decompression while sitting can be a nice help. However, “motion is lotion.” Perennial decompression is no better than perennial compression. Balance is crucial- https://b-reddy.org/2014/08/22/how-sitting-kills-your-knees/
Stephanie Lippencott
August 15, 2019
Love your detailed explanations. I’m a 54-year-old female with moderate pelvic instability due to L5-S1 anterolisthesis (congenital). I spend a lot of time studying anatomy & physiology in my spare time because I’m pretty sure in another life I would have been in the medical field and think the human body is fascinating. The chicken-and-the-egg question is always there for me as I want to understand how symptoms cascade from the root causes. Knee issues you’ve mentioned here, could derive from pelvic alignment, could they not? In addition to core work (I practice Pilates regularly), strengthening glutes med/min for me are a huge focus. That helps TFL and IT band relax a little, right? Love to understand the physiology so your comments would be appreciated. Thanks again.
b-reddy
August 16, 2019
Hey Stephanie,
The pelvis can influence the knees, sure. The anteversion section touches on that.
How you strengthen the glutes would be critical as to whether you are relaxing the TFL. If you say, are doing a ton of abduction work, the TFL is also an abductor, so you could very well be activating the TFL.