I’m going to reference Scapular winging: anatomical review, diagnosis, and treatments often.
–
Anatomy of scapular winging (muscular)
Serratus anterior
Of course, we have to start with this muscle.

The serratus anterior protracts and upwardly rotates the scapula.

Let’s use a nice quote from the paper to get more specific. Pictures and bolding from me:
“The serratus anterior is a broad flattened sheet of muscle originating from the first nine ribs and passes posteriorly around the thoracic wall before inserting into the costal surface of the medial border of the scapula.
(Fancy talk for it goes from the ribs to the scapula.)
The serratus anterior has three functional components. The superior component originates from the first and second ribs and inserts into the superior medial angle of the scapula. This component serves as the anchor that allows the scapula to rotate when the arm is lifted overhead.
The middle component of the serratus anterior originates from the third, fourth, and fifth ribs and inserts on the vertebral border of the scapula, serving to protract the scapula.
The inferior component originates from the sixth to ninth ribs and inserts on the inferior angle of the scapula. This third portion serves to protract the scapula and rotate the inferior angle upward and laterally.
As a whole, the main function of the serratus anterior is to protract and rotate the scapula, keeping it closely opposed to the thoracic wall and optimizing the position of the glenoid for maximum efficiency for upper extremity motion.”


It’s not just about the serratus anterior
The serratus anterior is not the only muscle impacting a winging scapula. When a scapula wings it’s because it isn’t held close to the rib cage. The serratus anterior gets a lot of attention because it’s anterior to the scapula, and attaches to the scapula. When a scapula wings it often displaces posteriorly. Naturally, the thinking goes the serratus anterior is “long and weak” because the scapula isn’ t being held close to the ribcage.
However, other muscles connect anterior to the scapula, and connect to the scapula.
Trapezius

Because the spine is ventral to (in front of) the scapula the trapezius can pull the scapula a bit anteriorly. That is, closer to the ribcage.
Parts of the trapezius also fall on top of the shoulder blade.

If the trapezius is on slack, or not firing properly, the compression on the scapula lessens. Making it more likely the shoulder blade won’t be as tight to the ribcage, aka wing.
Rhomboids
For many of the same reasons above, the rhomboids can play a role in the shoulder blade winging too. Because this is so rare (the authors go over this too), I’m not going to cover it.
Position of the scapula
Due to the attachment sites of the above muscles, we can get a good feel for which muscles need work by the position of the scapula. A nice chart from the paper:


Right scapula front view.

Right scapula back view.
Right shoulder winging due to issues with the serratus anterior (it gets progressively worse):
–
See how the scapula is traveling excessively medially and superiorly?


Winging due to issues with the trapezius:

From the paper: “Notice the lateral displacement of the scapula with the superior angle more lateral to the midline than the inferior angle.”
An important note here: I don’t think it’s feasible to fully separate these two impairments. When a serratus anterior issue is present it’s pretty much guaranteed there’s an issues with something like the trapezius. For instance, while this has serratus issues:
You can see issues with the trapezius as well. The superior angle (where the trapezius attaches) is lateral to the inferior angle. A sign the trapezius is also not firing like it should be.

–
Anatomy of scapular winging (nerve)
Long thoracic nerve
Much like the serratus anterior, of course we have to go over this nerve. The long thoracic nerve is part of the brachial plexus.

The brachial plexus is a group of nerves which run down from the neck, under the clavicle, connecting to various points around the shoulder. 
-Image credit and copyright to Kenhub (great anatomy site!)
The long thoracic nerve connects into the serratus anterior:


Because this nerve is what gets the serratus anterior to fire, and people with scapular winging often have so much trouble getting their serratus to work, the long thoracic nerve gets a lot of attention. However, attacking the nerve doesn’t get us anywhere. We need to go after why the nerve has a problem. Why is it having trouble firing, thus the serratus anterior is having trouble firing. The nerve doesn’t just sporadically stop working one day.
–
Figuring out the cause of scapular winging
“The serratus anterior is weak” is not a cause. “The long thoracic nerve isn’t working” is not a cause. Why are there issues with the serratus anterior? Why did it become weak? Why is it not firing properly? Why is the long thoracic nerve not helping?
Muscular
As I went over above, we’re primarily interested in getting the trapezius and or serratus anterior to work better. Muscles which help hold the scapula to the rib cage and lift (rotate) it upwards. With that, it’s logical to assume muscles which perform the opposite functions -pull the scapula away from the rib cage and or rotate it downwards- are likely working too much. Muscles such as, but not limited to, the rhomboids or pec minor. We want to calm them down. If they’re too active they can limit the ability of the trapezius and serratus anterior to do their jobs.
Nervous
We’re interested in anything which could limit the ability of the long thoracic nerve to fire. We’re primarily concerned with compression of the nerve. From the paper (when discussing the long thoracic nerve):
“Proposed vulnerable sites for injury include compression of the nerve between the clavicle and first rib and traction within the nerve’s fascial sheath.”
The clavicle and first rib may come closer together pinching the long thoracic nerve between them.

In my experience, this most often manifests with the clavicle / shoulder drooping.

Which goes hand in hand with our discussion of muscles pulling the shoulder down. The overactive muscles which may cause a shoulder to droop, are the same muscles which oppose the serratus anterior and trapezius.
This is the long way of saying you can’t really separate nerve issues from muscular issues. They work together. Granted, I once saw a woman who had her long thoracic nerve severed because of a mastectomy. Her winging was truly a nerve problem. But that’s the rare case. We’re more concerned with our average person.
So, how do these certain muscles become dominant? How does this nerve get compressed?
–
Daily activities causing issues with scapular winging
I’m going rattle off a bunch of scenarios where the shoulders are being depressed / downwardly rotated.
Bra Straps
The downward pull of bra straps can cause the shoulders to become depressed over time.

This is especially poignant for those who carry a considerable amount of weight in their bra.
Carrying heavy objects

Much like the bra strap comments.
Computer Posture
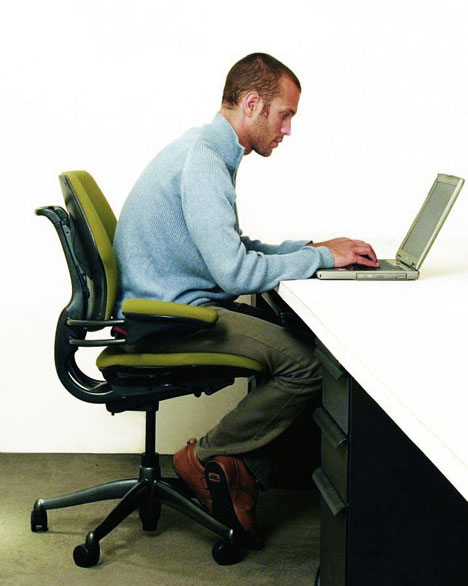
The forward head posture causes the levator scapulae (downward rotator) to pull on the scapula
The internal rotation (hands / arms turned down and in) can cause stiffness in the pecs and lats. Both of which can limit our ability to get our arms up.
Leaning on elbows

Notice the right shoulder protruding
This can push the shoulder into retraction, stiffening the rhomboids.

Next, this can indirectly cause winging. When leaning on the elbows the humerus can become displaced anteriorly (forward) and or superiorly (upward), lengthening the subscapularis.

A muscle which depressed the humeral head, pulling it posteriorly (backward) and inferiorly (downward).
When the subscapularis is lengthened it may shut down causing other humeral head depressors, such as teres minor and infraspinatus, to work more than they should.

These muscles can then stiffen up. This stiffness may appear when someone internally rotates their arm. Notice the winging during internal rotation here:

Credit to Diagnosis and Treatment of Movement Impairment Syndromes (Great book!)
I didn’t go over this in the initial anatomy section, but stiff external rotators of the humerus can cause winging as well. Because these external rotators connect 1) anterior to the scapula and 2) to the scapula, similar to the muscles I went over earlier. The difference being these muscles internally rotate the scapula (away from the ribs), while the others externally rotate it (close to the ribs).

–
Standing with hands on hips

This goes hand in hand with the above. The internal rotation causes issues with the lats and pecs, and the elbows behind the humerus promote anterior translation of the humeral head (stretching the subscapularis). All these muscles pull the arm downwards as well. Something we want to avoid in exercise too.

–
Exercise routines causing issues with scapular winging
Too much pulling
Exercises such as DB rowing, chin ups, lat pulldowns, chest supported row, all work on muscles which downwardly rotate and retract the scapula, as well as extend the humerus. Muscles like the rhomboids, lats, teres minor and infraspinatus. As we’ve seen, if anything, in someone with scapular winging we want to atrophy these muscles.
Too much work in horizontal plane
Horizontal meaning the arms move forward (in front of body) and back (behind body), rather than up (overhead) and down (below head).
Going with that, horizontal pushing exercises, such as push-ups, bench pressing, DB bench pressing, all work the pecs to a great degree. Muscles we again want to calm down.
Yes, it’s true some scapular protraction is present. But this is where we go back to the function of the serratus anterior.
“the main function of the serratus anterior is to protract and rotate the scapula”
And there’s minimal, if any, upward rotation in any exercise only taking place in the horizontal plane. Now we can see why something like the push-up plus exercise is pretty much futile.


Some people will lift the arms up a bit higher to place the shoulders in more of an upwardly rotated position. If you want to really upwardly rotate the scapula you know what you could do even more of? Lift the arms higher. Like, all the way up. Isn’t this the goal anyways? To be able to lift the arms all the way up?
Furthermore, exercises like the push-up plus and others may promote scapular protraction while simultaneously promoting scapular retraction.


–
Whatever you may be promoting in scapular abduction (protraction) you’re offsetting with adduction (retraction). Something you rarely want in a scapular winging issue, or most shoulder issues for that matter.
Note the similarities:
Pain during arm elevation due to excessive scapular retraction:
Looks pretty similar to the position of a push up plus:


Sure, you could cue around this (I rarely ever see someone do so), but you still have to account for the fact upward rotation is not being sufficiently attained.
Lack of overhead work
What you end up concluding is the way to solve these types of issues is not to avoid overhead work, but to embrace it. Overhead work enables us to:
- Fully utilize the serratus anterior and trapezius (upward rotators and preventers of winging)
- Stretch the pecs, lats, rhomboids, levator scapula (downward rotators)
- Stretch the infraspinatus and teres minor
This doesn’t mean you immediately start forcing your arm overhead. Some people need to very slowly work on their overhead range of motion. I’ve seen many a people who could only go a couple inches before their pain kicked in, and that’s ok. We don’t push into that pain, and we’ll see the range of motion improve with time.
Forcing me to disagree with this statement from the authors:
“Upon diagnosis, patients should be advised to avoid overhead use of the effected extremity and to avoid activities that cause pain.”
It’s not so much what you do, but how you do it. It’s not so much you shouldn’t bring your arms overhead, it’s how you go about doing it.
You’ll never be able to get your arms vertical by only working them in the horizontal.
–
If you’re looking for some other steps you can take to help with scapular winging, specifically during the day, such as while typing and sitting, you may be interested in this.







{kind=link}
{kind=link}
Wendy
December 29, 2014
Brian, my daughter is a 15 year old competitive soccer player who suffered a concussion due to an overinflated soccer ball to the head back in August. She has had headaches every day since then. Pain ranging from 3-9(on a scale of 1-10). We have been to 2 PC MD, neurologist, chiropractor, neurologic chiropractor, PT, accupressurist and have found no relief. MRI came back normal. Medical doctors say it is PCS(post concussion syndrome). Practitioners who have actually had their hands on her have told us she has reversed curvature of her spine starting in her neck, tight scalenes and a disruptive nerve pattern in her upper scapular area – winging, causing her headaches. However no one can tell me how to help her. She hasn’t worked out since the injury and when she attempts she gets either nauseous or a painful spike in her headaches. Thoughts?
reddyb
December 30, 2014
Hey Wendy,
Few thoughts-
-It can take quite a while for some people to get over a concussion. The professional sports world hasn’t helped here, as so many of these athletes are back on the field in a couple of weeks. In reality, not much heals that quickly. Concussions seem to have quite a variance. I believe I’ve seen some people report symptoms for a year, if not longer.
-My initial thought would be things are tied to the concussion, based on the timeline of things. That is, if her musculature / movement and whatnot were causing headaches, I’d assume some manifestation before the concussion.
-That said, sometimes an injury can make dysfunction manifest more nefariously. (I talk about this some in reference to a car accident, here: http://b-reddy.org/2011/06/02/example-of-impaired-movement-causing-pain/ ) There have been some ties to headaches and things like forward head posture. So, there could be something worth working on here.
-I’d do some gentle, relatively easy movements, so that the muscular / nerve / movement side is being addressed BUT she’s not overworking her likely still healing brain. (I’d also work on things which lessen the tension on her neck, such as some of the things I go over in this post. (Not holding a purse on one arm, e.g.))
Lastly, I actually just came across this article two days ago, mentioning how some time away from physical and mental activity can help concussion healing: http://natmonitor.com/2014/12/19/concussion-healing-with-dramatic-results/ (There are some interesting things regarding supplementation you may want to entertain as well.)
This is a better, more thorough write up on that study: http://www.momsteam.com/cognitive-rest/new-study-shows-benefit-cognitive-physical-rest-in-concussion-recovery
I will say, while concussion healing is beyond my knowledge, in every other realm of healing, movement is paramount to getting the process going. Where something like bedrest is often quite detrimental. Again, the bran is different, but I’d be surprised if complete rest was optimal here. In my experience, the dosage is what’s most important. When someone sprains an ankle you don’t have them keep on running, but you do have them perform so low level exercise still. I’d be surprised if the brain was any different.
I think the points that article brings up regarding letting, especially a teenager, rest from things like the black mirror (screens), make a lot of sense though. Nowadays this seems even more applicable as a teenager’s brain is so constantly being bombarded by stimulation.
Hope that’s helpful.
cliff graves
February 19, 2015
Hi, absolutely love your knowledge and never really viewed it like this before. I appreciate it has been a while since the last comment made but only just came across this fantastic article. My question is could a near vertical angled handstand push up (from an anatomical standpoint) activate the necessary muscles of upward rotators as opposed to downward rotators? hoping, you will respond soon. Love your site. Gratefully, I await in anticipation.
reddyb
February 19, 2015
Hey Cliff,
Thanks for the nice words.
To answer your question, yes. The potential issue though is what’s going on with the lower back during the handstand. It’s common to have a significant amount of lower back extension during a handstand, which diminishes how much something like the latissimus dorsi is being stretched during the exercise. So, while you may get good upward rotation activation, you *may* not get downward rotation relaxation as much as you want.
In my experience, in those with shoulder flexion / upward rotation issues, getting only their arms overhead is difficult enough. Throwing an entire bodyweight on that isn’t going to happen, at least not for a while.
So, the context is crucial here.
I discuss the lats and the lower back some here, if interested: http://b-reddy.org/2011/08/04/3-common-tight-muscles/
cliff graves
February 20, 2015
thanks……
Jo
March 12, 2015
Hello!
I came across this site researching scapula winging and I have to say it’s the best explanation ive found anywhere!
I’m 23 and my scapulae have winged for as long as I can remember – when I internally rotate my shoulders so that my hands are behind my back, it looks the same as the girl in the picture; you can grab on to pretty much the whole inferior medial border of my scapulae.
I am normally pain free but have big trigger points under the medial border on both sides which sometimes cause me a lot of pain through my shoulder, upper back and neck. Is this likely to be due to instability from the winging?
I gather from your article that it is also common to have pain and difficulty raising the arms above the head – I have no problem with this currently, am I likely to develop this sometime if I don’t do something about correcting the condition?
Thank you!
reddyb
March 16, 2015
Hey Jo,
If you only have winging in that one circumstance, then you may not have much to worry about. Where that discomfort in your mid-back could be from something else. That’s a common area to have some discomfort in time to time in general. Doesn’t necessarily mean anything needs to be changed though. Could be you had an awkward night of sleep, sat at a desk too long, etc.
That said, the winging can definitely pull on the musculature in that area in some aberrant ways, causing some discomfort. So it’s possible.
As long as you maintain your ability to raise your arms overhead, you’ll probably be fine in that regard. If your shoulders do wing a good amount when raising the arms, or lowering them, then it’s worth working on. But just because your shoulder blades poke out a good amount when internally rotating them doesn’t necessarily mean they do that during other arm motions.
Sorry to be so vague here.
Cheryl
May 5, 2015
I have winged scapula. Had surgery for thoracic outlet syndrome. Damaged long thoracic nerve. Oct 2014. Im in severe pain my scapula comes completely out of my rib cage. I cant keep living like this. Do you know anyone that can help me. My Dr is researching trying to find me help also. I have muscles that have astrophy. 🙁
reddyb
May 5, 2015
Hey Cheryl,
You’re welcome to take a look at this: http://b-reddy.org/2013/06/20/the-remote-client-process/
Beyond that, where are you located?
Adam
June 27, 2015
What could be the causing of tingling and burning pain next to scapula’s border? It happens when I do overhead or arm rotating activities (washing the dishes for example). I may have winging scapula
reddyb
June 30, 2015
Winging scapula is one such potential cause. Not the only one though.
Crystal
June 29, 2015
I HAVE RECENTLY NOTICED THAT I HAVE A RIGHT WINGED SCAPULA I BEGAN NOTICING IT BECAUSE ABOUT 3 YEARS AGO I STARTED NOTICING ALOT OF DISCOMFORT IN MY UPPER BACK AND NECK ON THE RIGHT SIDE I HAVE TRIGGER POINTS IN MY MIDDLE TRAPEZIUS AND RIGHT DOWN BELOW IT I HAVE CONSTANT DISCOMFORT WHEN I LEAN AGAINST A WALL AS THEY DESCRIBE MY RIGHT SCAPULA COMES OUT MY KNECK MUSCLES ARE TENSE I GET CONSTANT TENSION HEADACHES AND CONSTANT MUSCLE TENSION ON MY RIGHT SIDE IT HAS GOTTEN WORSE OVER THE LAST FEW YEARS WHEN I TAKE DEEP BREATHES I FEEL PRESSURE ON MY ENTIRE RIGHT SIDE I AM NOT SURE IF THIS CAN HAPPEN DUE TO HAVING CONSTANT TENSE MUSCLES ON THIS SIDE I GET CHEST PAINS UNDER MY ARMS RIGHT BEHIND MY TRIGGER POINTS THAT CAUSE THE CHEST PAINS I BELIEVE NOT SURE THOUGH I HAVE VERY BAD POSTURE DUE TO A ACCIDENT FROM A 3 STORY FALL WHERE I LANDED ON MY FEET AND IT CAUSED A HAIRLINE COMPRESSION FRACTURE TO MY L1 WHICH I WAS REQUIRED TO USE A BACK BRACE THAT PUT ME IN A CONSTANT HUNCHED POSITION ABOUT 8 YEARS AGO I STARTED NOTICING THIS ISSUE AFTER I HAD MY LAST CHILD ALMOST 4 YEARS AGO I HAD GAINED ALOT OF WEIGHT AND HAD ALOT OF WEIGHT ON MY CHEST WHICH I FELT STARTED THIS PROBLEM BUT BECAUSE ITS PERSISTED FOR OVER THESE YEARS AND I NOW HAVE A WINGED SCAPULA I CANT STOP WORRYING IT IS MORE THAN WHAT IT MAY SEEM. PLEASE DO YOU HAVE ANY INSIGHT AS TO WETHER THESE SYMPTOMS ARE RELATED TO POSSIBLE POSTURE MUSCLE PROBLEMS, CAN YOU GET CHEST PAINS AND FEELING OF PRESSURE WHEN YOU TAKE DEEP BREATHES ON THAT ENTIRE SIDE MY RIGHT SIDE IS MY DOMINANT SIDE I SLOUCH VERY BADLY AND MY RIGHT SIDE LEANS DOWN MORE THAN THE LEFT ALL MY ISSUES ARE ON THIS SIDE. I SEEN A DOCTOR AT AN ER ABOUT 6 YEARS OR SO AGO AND THEY TOLD ME I HAVE MUSCULOSKELETAL FRACTURE WHICH I BELIEVE WAS IN THE SAME AREA BUT DIDNT NOTICE THIS PAIN UNTIL AFTER MY SON….PLEASE I NEED SOME ADVICE AND SOME OPINIONS IF THIS IS NORMAL AND WHAT I NEED TO DO
reddyb
July 1, 2015
Issues with headaches may be related. Chest pains I’m not sure about. I’d have to take a closer look at you.
In terms of what to do with winging, the low shoulder, etc., there are a lot of recommendations in this article and the comments.
DL
August 15, 2015
I believe I have a winged right scapula, and it causes constant discomfort between the scapula and the spine. The only way to relieve it is to anteriorly rotate my shoulder as if I’m about to check somebody into the boards. Also, when I’m standing up straight, the bottom of the scapula bulges out and my right shoulder droops. What would be your recommendation to help remedy this issue?
reddyb
August 18, 2015
Hey Doug,
Did you see the recommendations in this post and the comments?
Carlee
September 25, 2015
Brian,
I’ve been burning through your posts for about a week now and I must thank you for all the great info and practical applications you present. I’ve got a few significant issues I’m working on that you’ve helped me conceptualize better.
I won’t even go into my R external tibial torsion/femur internal rotation/dead butt syndrome issue, though you’ve helped me there; until very recently, my most frustrating issue was what was diagnosed ten years ago as ‘thoracic outlet syndrome’. I’m sure you’ve encountered this syndrome at least once with a client. I experienced pain, then tingling/weakness/numbing, to deadness in my R shoulder and down my R arm when performing any aerobic activity or seriously repetitive overhead R arm movement lasting longer than about 7 minutes. I was in the AF, so I did a lot of compulsory running in great pain with one arm flopping around like an attached dead fish. Not cool. Anyway, I almost had exploratory surgery- and that would have been a huge mistake and would not have improved my situation, given what I now know. I think a better term for my problem is ‘multiple crush syndrome,’ a term you won’t see a great deal about in recent literature because it implicates fascial nerve tractioning (in one or more areas- *multiple), which is not something on which you can perform surgery to remove or repair or prescribe medicine to dissipate. Fascial tractioning, if you aren’t familiar with it, is a phenomenon in which nerve fibers get adhered or entrapped in the fascial sheaths they run under, through, or over. If, like my massage therapist discovered in my case, certain muscles become hypertonic chronically due to muscular compensations for trauma or bad posture or incorrect training, the tight –contracteded– muscle tissue won’t fully relax or contract, and so won’t efficiently move waste products out and nutrients/fluids in. These muscles become starved, dry, sticky, and tender versions of their formerly robust selves, and that ‘stickiness’ translates to the fascial, which then tractions nerves. Or that’s my best understanding. All super technical terms- especially ‘sticky’.
Anyway, my posture was just off enough (shoulders rolled forward, thoracic spine excessively kyphotic/ribcage caved in, abs and serratus anterior offline), that my muscles compensated (pec minor clamping the corocoid process down hard for stabilization, levator scap and upper traps doing their damndest to hold my scap in place, scalenes and SCMs tight and impenetrable, ant delt and bicep like rocks), and caught up some nerve fibers that passed through them and down my arm. My massage therapist put me through some intense myofascial release and freed up one site of fascial nerve entrapment after another. Let’s just say, it was a lengthy process, my time on the massage table was very uncomfortable (but not painful!),and the temporary nerve inflammation that followed freeing a portion of a tractioned nerve was at times excruciating (for about two weeks after Tom released one in my arm, having my R hand even lightly squeezed would bring me to my knees –very awkward when shaking hands– and after he finally got the tractioned nerve in one of my R scalenes released, my R scap felt like it was on fire for a solid week). All the discomfort was worth it, though; last month, for the first time I can remember, I ran for fifteen minutes straight without even a twinge of pain, tingling, numbness, or deadness in my R shoulder and arm!
The reason I share this long, convoluted story full of parentheses is you talked about massage therapy dismissively, and I understand why you don’t appreciate its value in a rehab program, probably because you’ve never interacted with a good massage therapist as opposed to a spa masseuse. There is value to massage therapy, especially with clients with issues like you encounter- as evidenced by my own experience and countless others I’ve witnessed in my short time as a massage therapy student. I think combining the work you’re doing with massage therapy could be synergistic. Also, if you’re having a hard time pinning down all the muscular/fascial links in a client’s chain of disfunction, get them to a massage therapist and ask for a report on their palpation findings- you will not believe how easy it is to learn a person’s muscular imbalances and areas of pain with your hands, and not a verbal clue given by the client!
I have an eight-year history as a super-part-time aerobics instructor –and at one time, ACSM certified personal trainer– so I know that my pain was caused by my messed-up posture and my messed-up movement patterns, and only changing those will provide me with long-term freedom from pain and disfunction.. Massage therapy released my nerve traction sites, but if I continue to move as I always have, I’ll probably develop new entrapments and experience new pains. So I’ve taken what you’ve posted and added it to my rehab- I thank you! Please take what I’ve shared with you and consider using it, too. I think you’ll be pleasantly surprised.
Also, that mother who posted about her daughter suffering pain following a soccer-related traumatic head injury should consider that the musculature of her daughter’s neck is probably locked down protectively like after suffering whiplash, and even if the original injury/concussion has healed (and maybe it hasn’t yet), the body can and often does retain compensatory/protective patterns –because the nervous system is nervous, haha– I don’t believe MRIs will show sites of nerve entrapment/tractioning, or even give insight into muscle tonicity. She could have developed issues similar to mine (nerve tractioning with referred pain down the nerve(s)) or just the tension in the neck could translate down a tightened levator scap to the scapula or up to the occiputalfrontalis muscle/fascial sheath that stretches from the back of the head to the forehead. I can’t tell you how many people come into clinic with tension headaches and leave without tension headaches, because we warm, stretch and loosen that occiputalfrontalis sheath and its immediate fascial-sheath-sharing neighbors. It’s like magic-but it’s not. She should definitely consider giving a good massage therapist a crack at the pain. If nothing else, the therapist might be able to offer some insight from palpation that most other professionals just can’t give- a massage therapist is much more sensitive than the average PT when it comes to palpation because feeling tissue is what we do day-in, day-out, and most PTs I’ve interacted with seem nervous just laying a finger on a glute for two seconds! Most progressive (not stuck-up) PTs and Chiros know a few good local therapists –or employ them– and will refer. My therapist in particular is recommended by several doctors here, and has had great success with people recovering from whiplash, major car accidents, sports injuries, traumatic head injuries, etc..
reddyb
September 29, 2015
Hey Carlee,
Thank you for the nice words.
-What you’re describing sounds like the Anatomy Trains philosophy. I’m quite familiar with it. I’ve written about it a few times, recommend the book, and have met and seen Tom Myers (a world renown massage therapist who popularizes the philosophy you’re talking about) speak in person- http://b-reddy.org/2013/10/08/a-day-with-tom-myers-of-anatomy-trains/
-I think you may have mistook my comments on massage therapy. I never dismissed it as not valuable, nor I have ever said people don’t get anything out of it. I write how someone could derive benefit from it here, along with other comments: http://b-reddy.org/2015/02/02/recovery-modalities-whats-worthwhile-along-with-some-massage-discussion/
-My main issue with massage therapy is the thing you admit is an issue in this comment. What do you do after the massage? If you go back to all the same habits of before, you likely end up feeling like you did before. Massage therapy is therefore a symptom modality, not a cause modality. That doesn’t mean it can’t be valuable, but it does mean it’s a band aid. Band aids can help, but what’s causing the cut?
-> Similar to drugs, band aids can also be detrimental. Where rather than go after the cause, people instead go after the symptoms, as it often requires less work on their end. “Let me pop a pill rather than X.” “Let me go to the chiro rather than figure out why I regularly have to go to the chiro.”
-I’m not sure about using palpation as a guide to dysfunction. At least much of what I’ve seen with this, the assumption is “if it’s tender it’s tight,” but that’s not true. If it’s tender, it may be *long* (typically meaning strained) as well. Furthermore, palpation is then like posture, while it may be a window into how someone is moving, it’s no guarantee. You still need to watch the person move.
I can see palpation being helpful with something like noticing a particular muscle is hypertrophied (how will a massage atrophy a muscle? or hypertrophy one?), but in most cases, you can see this as well. Again, doesn’t mean there is *no* value there, but I’m not sure the value is what many think it is, nor am I sure it’s applied correctly.
Jackie
January 3, 2016
I developed winged scapula after a chiropractor herniated 2 discs in my neck. I have constant spasm and pain in between shoulder blades, neck and ribs. I’ve tried everything and nothing works. My EMG is normal but doctors expected an abnormal reading. It is affecting every aspect of my life. Please some advice.
reddyb
January 5, 2016
Hey Jackie,
Sorry to hear about your injury. In terms of advice for the scapula, this post and the comments has quite a bit of it. Not sure what else you’re looking for?
Mike
January 5, 2016
I’m big into lifting weights/bodybuilding. I’ve known since maybe 2010 (1 year into lifting, a few years into working out) that I had some upper crossed and lower crossed syndrome going on. Most notably upper. I browsed around online and figured that it was just from being better/stronger at pushing exercises than pulling exercises. Most sources talking about ’rounded shoulders’ don’t go into too much detail. They mainly say do less pushing, do more pulling. Up the dose on things like rear delt flys, face pulls, and rows for the rear delts, lower/mid traps. Lats, pecs, anterior delts, and upper traps are the muscles that promote rounded shoulders. These are things I’ve been incorporating in recent years. My lats and chest are definitely my most developed muscle groups.
Fast forward to recently I felt something wrong in my lat and went to the PT.
(Quick backstory on lat. Not sure if this is related but in 2012 I was doing low bar squats without great shoulder mobility and I felt a burning sensation near my scapula that only intensified the longer I had the bar there. I didn’t notice anything for a while. Then in 2014 I was in the middle of a banded lat stretch that I was probably putting way too much force into and I felt an immediate burning feeling in the lat. I thought I strained/tore something in there. And any time I tried to forcefully stretch my left lat after that, I’d get a burning sensation that would quickly get worse and worse the longer I held it. But I never felt it outside of that. I lifted normally because I didn’t notice anything. One day for some reason I did some light 10 second static lat stretches prior to lifting and felt a tweak in my one lat after pulldowns and face pulls which I thought tore something small in there. I stopped all upper body lifting to rest it. It didn’t really hurt after the first couple days or anything but it felt like something was wrong in there. I stopped all upper body lifting for a couple months, then went to the PT).
Anyways, the PT thinks it’s just that my left scapula has some winging going on that caused it over time. Nothing drastic. They did shoulder mobility tests and like I always knew (even prior to the lat thing), my shoulder posture/mobility wasn’t the greatest. They did some deep tissue massaging in the lat and had me do some basic things like the sleeper stretch, banded rows with a hold, and an overhead wall stretch where you’re facing the wall on a daily basis. He basically only said to lay off the pushing exercises and lay off the shrugs. Which is something I’ve always seen/read online. So I’ve been back for 8 weeks so far and have just been doing 3 upper body workouts a week constantly going for progressive overload. Mainly seated rows, chest supported rows, face pulls, rear delt flys, lateral raises, curls, and extensions.
HOWEVER I just came across this article and I see you said that too much pulling, especially horizontally, is one of the major problems. This has totally thrown me off course because horizontal pulling is basically my staple first couple exercises (mid/lower traps). My understanding before was that vertical pulling, vertical pushing, and horizontal pushing primarily work the lats/chest/anterior delts which all hurt posture. Like I mentioned before, most sources I come across just say to add in more volume on things like face pulls and rear delt flys.
What would you advise for someone into bodybuilding? Drop all compound lifts and focus only on corrective work? Should I lift normally across all planes (instead of just horizontal pulling like I’ve been doing) and add in proper corrective work with more volume? It already KILLS me inside that I’m not lifting more balanced like I usually do. Right now I rarely feel the lat thing but I know my shoulder posture still isn’t perfect. I can see looking from the side that my left shoulder is slightly more rounded than my right. No pain or anything though. Also, I recently switched jobs and don’t have health insurance for now, so I can’t go back to the PT.
reddyb
January 5, 2016
Hey Mike,
Give this a read. Might be exactly what you’re looking for, at least in the general sense: http://b-reddy.org/2014/07/20/bodybuilding-programming-issues-and-dealing-with-stubborn-clients/
If you want to get really specific, I do offer remote services: http://b-reddy.org/2013/06/20/the-remote-client-process/
Nice email by the way!
john
March 16, 2016
Hi brain back in jan 2015 I pushing in a 375pound wall oven . I thought I torn lat. muscle in june I was daig. With winged scapula I’ve has emg and mri doctor doesn’t know what is causing problem any idea thank you john
reddyb
March 18, 2016
Hey John,
If you have a winging scapula, my idea would likely be what’s in the article. If you want specific help, you’d have to check this out: http://b-reddy.org/category/pain-2/shoulder-pain/