From an upcoming, much longer post, detailing my second visit to The Washington University in St. Louis. Where I took a course by Shirley Sahrmann and the physical therapy department. You can read about my first visit here.
Shirley made some remarks on how past meniscal issues can affect current knee alignment.
When it comes to the meniscus, medial issues are more common than lateral issues.

Medial meniscus on left; lateral meniscus on right. (Right knee, top view.)

Right knee, anterior view. (Adapted from http://www.sportsorthopaedicspecialist.co.uk)
When you’re dealing with an older demographic, if they have had a meniscus issue, they probably had a tear which was left alone, or a partial menisectomy. Within that, it was probably on the medial side. Mensical repairs are a newer procedure, and most older people had their meniscal surgery done decades ago. Thus, it was probably a partial menisectomy. (This is worth knowing because most clients won’t remember or know what specifically was done to their knee.)
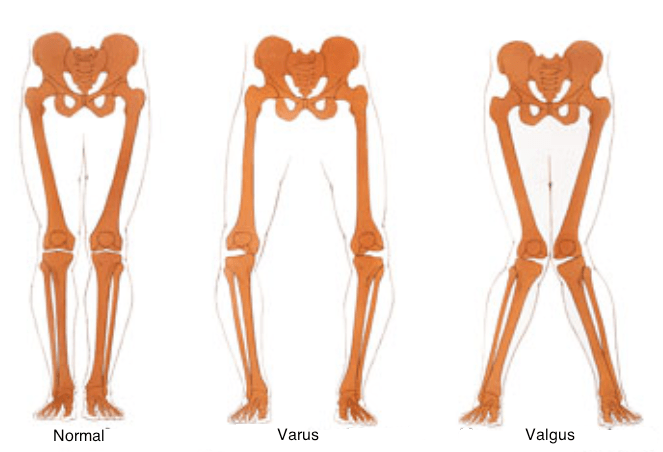
What you may see with a person like this, especially as they age, is their knee alignment changes to reflect their meniscal changes. Because the medial side has lessened or is gone, the femoral condyles don’t sit on the meniscus like they used to. The person may shift to a varus alignment.
To illustrate this, I’m going to show an example of someone who had their entire medial meniscus taken out. This is often not the case, but it helps for clarity. Because this is tough to visualize, at least it is for me, try using a cup with a ledge to help. One side of the ledge is the intact meniscus, the other is the excised:

You can see how things will change:
Lateral meniscus left in tact; medial meniscus has been removed.
Close up of normal alignment (right leg, anterior view):

Close up of varus alignment:

Note the similarities:


This can go the other way too: Lateral meniscus excision => Valgus alignment. In fact, I have a client with this deformity. Can you recognize which knee had the lateral meniscus partially excised?

The right:

Using the cup again:


There’s that sharper angle at the knee joint now:
![]()
![]()
This is important because you gain an increased understanding of why someone looks and moves the way they do. While I focus with Sharon (pictured above) on not letting her knee cave in, we both understand not to expect it to look like her other knee. We also understand her knee having this now structural issue, predisposes her to not handle certain activities well. Like the racquetball she loves to play. Having a knee with an increased valgus alignment makes her more susceptible for it to collapse inward during activity, which is often how knee injuries happen.
This is the conundrum with many meniscal procedures. While they may give you pain relief in the short term, helping you get back to the activity which likely caused your injury -racquetball for instance- the meniscal procedure could very well make it more likely you injure your knee again, like while playing racquetball.
–







Posted on February 24, 2014