A mindset I’ve been trying like hell to get people out of is the, “Long =weak; short = strong” muscle view. Where people go, “Ok, this is tight, it must be too strong; I need to stretch it and not strengthen it. Ok, this is weak, it must be too long; I need to strengthen and shorten it.” In a lot of instances, this is true. Not every instance though.
For this post, I’ll ignore the fact this mindset doesn’t include how everything works together (how everything moves), which is what actually matters. Strengthening a bunch of individual muscles and stretching a bunch of other individual muscles gets you as far as Leo at the Oscar’s. You get to be in the conversation, but then you’re D.O.A.
A prominent example illustrating the flaw in something like “This is tight; it’s too strong,” is the gluteus maximus. Atrophied (weak) glutes are readily apparent while standing.
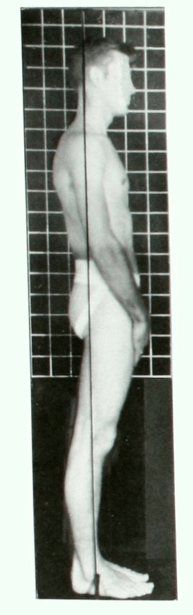
Picture from Kendall’s “Muscles: Testing and Function, with Posture and Pain.”
What’s also readily apparent, is many with atrophied glutes are standing in hip extension.

The glutes are hip extensors. If the hip is in extension, the gluteus maximus is shortened, not lengthened. Yet, they’re atrophied. The muscle is shortened and weak at the same time? Yes.
Muscles contract using filaments, which latch onto one another.
-

Shorten, shorten, shorten, lengthen. (GIF made from this cool video: http://www.youtube.com/watch?v=0kFmbrRJq4w )

If these filaments are significantly shortened, they can’t as effectively contract. There’s nothing left for them to latch onto. They’re at this point in the above clip:

No more room to contract.
If they’re chronically, excessively shortened, the muscle can’t do much, if any, work. It can’t produce much, if any, tension (length-tension relationship), leading to atrophy.

We’re focusing on the left side of the graph right now.
It’s like when someone gets casted up. The muscles in the cast have a hard time producing any tension. Hence the atrophy once the cast is removed.
Furthermore, if a particular muscle can’t do the work it’s supposed to, other muscles pick up the slack. This is why it’s so common for someone whose glutes are atrophied to have lower back issues. Their lower back is trying to pick up the slack. You see the same thing with hamstring issues. If the glutes aren’t extending the hip like they’re supposed to, other muscles which can have this influence will try to help. Like the lower back and hamstrings.
Some might be thinking, “But aren’t the hamstrings, who extend the hips too, also excessively shortened in this case?” Not usually. Because when the hip is in excessive extension, the knee often is too.

And the hamstrings extend and flex the knee. While they have been shortened into hip extension, they’ve been lengthened into knee extension. The rubber band has been tautened from one end but slackened from the other. The filaments aren’t on top of one another like they are at the glutes. In fact, with atrophied glutes often come hypertrophied hamstrings (and spinal erectors).
In someone like above, it’s common to see the atrophied glutes, see the lack of gluteal contraction during an assessment, and prescribe a bunch of glute exercises. Exercises usually involving a great deal of hip extension. 1) You better make sure the glutes are indeed helping the hip extension. Just because the hip goes into extension doesn’t mean the glutes are working. 2) How much hip extension does this person need? They already have plenty of it. You better make sure you’re not going into excessive extension, along with doing other things to work them back into some hip flexion. Their hips need to be flexed a bit before their glutes can effectively produce tension!
This is why it’s typical those with an anterior pelvic tilt have good gluteal definition.


The extra hip flexion can help the glutes produce more tension. Notice the caption in this graph from ExRx.net:
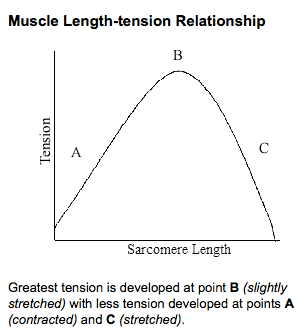
When the muscle is “slightly stretched” is when it can produce the greatest force. An anterior pelvic tilt can slightly stretch the glutes, leading to greater tension ability, leading to hypertrophy. While significantly shortened glutes often become atrophied; slightly lengthened glutes often become hypertrophied. Shortened, or tightened, muscles aren’t always strong, and lengthened muscles aren’t always weak. Sometimes, the opposite is true.
–






Den
March 3, 2014
Another excellent post. You explained how the first case should build glutes to reduce the issues around standing in Hip flex all day. But in the second post, if you stand in Hip Flex and have active Glutes how do you counter that?
reddyb
March 5, 2014
Hey Den,
Little confused on what you’re saying. In the first person above, the person standing in hip extension, I just want it to be clear I’m arguing not for them doing a bunch of stuff to build their glutes, but for them to first get out of hip extension.
Second, are you asking in someone who has an anterior pelvic tilt, but good gluteal definition, how do you work on the anterior pelvic tilt? If so, the external obliques are a good muscle to go after. In other words, whenever the person moves, don’t let them have an anterior pelvic tilt! (Worry about this more than you worry about what muscle to work.)
Simple, low level example: http://www.youtube.com/watch?v=iY3lmig5fKw
Joe D.
March 4, 2014
How do we prevent going into hip extension while exercising to strengthen the glutes? Or do we just avoid hyperextension? Thanks for another great post!
reddyb
March 5, 2014
Hey Joe,
I like to extend the hip without placing it into extension. A Bird Dog is one of my favorite ways to do this. The hips start in flexion. When you straighten the leg the hip is extending, but I often have the person keep their foot on the ground, so their hip doesn’t go into extension. It doesn’t go past 0 degrees. The way I classify it is 10 degrees past neutral is extension, and anything more than that is hyperextension.
The Bird Dog also insures the hip is moving without the lower back moving. Where if the lower back is stationary, it’s going to be pretty damn hard for the glute to not be doing any work.
Hope that makes sense.
Den
March 5, 2014
Brian, excellent response, to the my vague question. Excellent use of video, I like it!
So in the second part of your answer you are suggesting use the PSOAS major to do some kind of hip tilt then do the leg slide? As per my previous request, I look forward to reading a post or Ebook on Core or Ab exercises, I am sure you would do a great job of it.
I understand you comment about removing APT from all movement, but it’s kind of difficult to focus in that when walking or cycling. Standing or weights, yes I can see that working.
reddyb
March 6, 2014
In the Heel Slide video the external obliques and abdominals are what’s really generating the posterior tilt. From there, due to the nature of the slide, and you can cue someone to push their foot into the floor too, the hip flexors aren’t doing any work. On the way out, the hip extensors and quads are doing some work; on the way in the hamstrings and calves are actually working. Because the foot is being pulled into the ground, the direction of force precludes the hip flexors from generating much force, which is on purpose. There’s less compression on the spine this way, and it’s just easier than when the foot is coming off the ground.
With something like walking it can definitely be harder to prevent anterior pelvic tilt. Something simple though, like consistently placing one hand on your stomach to remind you to pull things up and in, can help though. Taking breaks to stand with your back against a wall can help too. That is, if your lower back is flat against the wall, you know you’re not in an APT. This can increase the person’s understanding of what an excessive lower back arch is.
Haven’t forgotten about your ebook idea. Got some other stuff (hopefully soon) coming first!